

Prognostic burden of heart failure recorded in primary care, acute hospital admissions, or both: a population-based linked electronic health record cohort study in 2.1 million people
- PMID: 28008698
- PMCID: PMC5420446
- DOI: 10.1002/ejhf.709
Prognostic burden of heart failure recorded in primary care, acute hospital admissions, or both: a population-based linked electronic health record cohort study in 2.1 million people
Abstract
Aims: The prognosis of patients hospitalized for worsening heart failure (HF) is well described, but not that of patients managed solely in non-acute settings such as primary care or secondary outpatient care. We assessed the distribution of HF across levels of healthcare, and assessed the prognostic differences for patients with HF either recorded in primary care (including secondary outpatient care) (PC), hospital admissions alone, or known in both contexts.
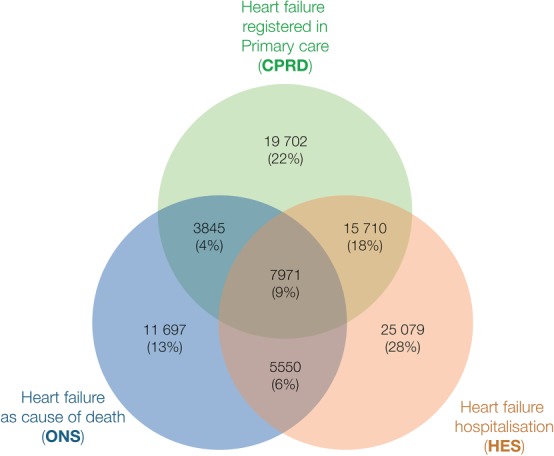
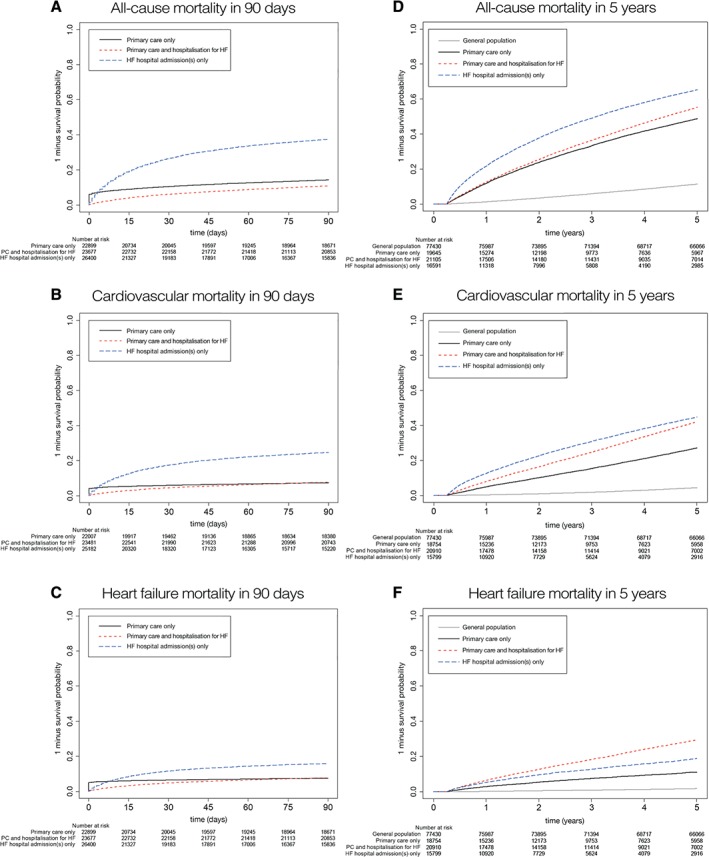
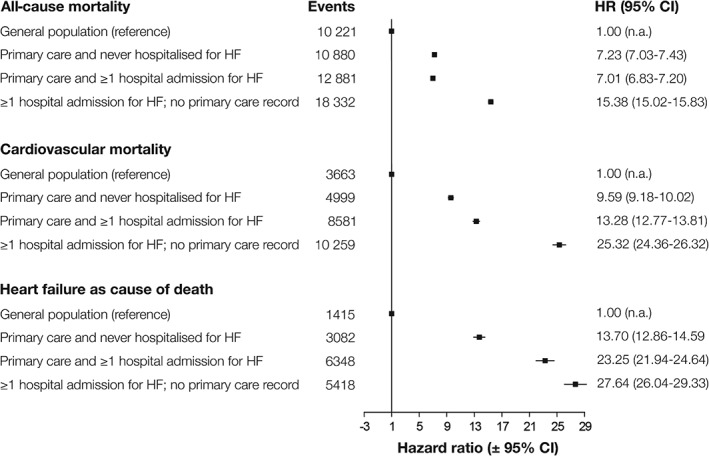
Methods and results: This study was part of the CALIBER programme, which comprises linked data from primary care, hospital admissions, and death certificates for 2.1 million inhabitants of England. We identified 89 554 patients with newly recorded HF, of whom 23 547 (26%) were recorded in PC but never hospitalized, 30 629 (34%) in hospital admissions but not known in PC, 23 681 (27%) in both, and 11 697 (13%) in death certificates only. The highest prescription rates of ACE inhibitors, beta-blockers, and mineralocorticoid receptor antagonists was found in patients known in both contexts. The respective 5-year survival in the first three groups was 43.9% [95% confidence interval (CI) 43.2-44.6%], 21.7% (95% CI 21.1-22.2%), and 39.8% (95% CI 39.2-40.5%), compared with 88.1% (95% CI 87.9-88.3%) in the age- and sex-matched general population.
Conclusion: In the general population, one in four patients with HF will not be hospitalized for worsening HF within a median follow-up of 1.7 years, yet they still have a poor 5-year prognosis. Patients admitted to hospital with worsening HF but not known with HF in primary care have the worst prognosis and management. Mitigating the prognostic burden of HF requires greater consistency across primary and secondary care in the identification, profiling, and treatment of patients.
Trial registration: NCT02551016.
Keywords: Acute hospital admission; Electronic health records; Epidemiology; Heart failure; Primary care; Prognosis.
© 2016 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Comment in
-
Integrating electronic health records into the study of heart failure: promises and pitfalls.Eur J Heart Fail. 2017 Sep;19(9):1128-1130. doi: 10.1002/ejhf.878. Epub 2017 May 25. Eur J Heart Fail. 2017. PMID: 28544192 No abstract available.
References
-
- Van Riet EES, Hoes AW, Limburg A, Landman MA, Van Der Hoeven H, Rutten FH. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion. Eur J Heart Fail 2014;16:772–777. - PubMed
-
- Rothwell PM. External validity of randomised controlled trials: ‘to whom do the results of this trial apply?’ Lancet 2005;365:82–93. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
