

There is Significant Practice Pattern Variability in the Management of the Hospitalized Ulcerative Colitis Patient at a Tertiary Care and IBD Referral Center
- PMID: 28009685
- PMCID: PMC6658167
- DOI: 10.1097/MCG.0000000000000779
There is Significant Practice Pattern Variability in the Management of the Hospitalized Ulcerative Colitis Patient at a Tertiary Care and IBD Referral Center
Abstract
Background and goals: Despite published clinical guidelines, substantive data underlying the approach to the management of hospitalized ulcerative colitis (UC) patients failing outpatient therapy are lacking. Variability in practice is therefore not uncommon and may impact clinical outcomes. The degree of variability, however, is not well-studied. Our aim was to evaluate variability in management of the hospitalized UC patient to inform future efforts targeting care optimization for this high-risk population.
Study: An internet survey was distributed among inflammatory bowel disease providers, which included: (1) nonvignette-based questions assessing provider demographics, experience, and practice setting; (2) diagnostic and therapeutic practice patterns based on a vignette of a hospitalized UC patient. Descriptive and univariate analyses were performed.
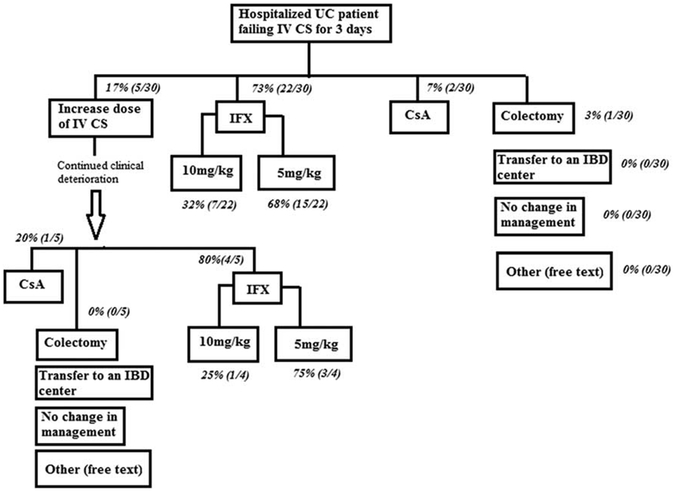
Results: Ninety-one percent of eligible individuals were included. Nearly 97% endorsed confidence in management of hospitalized UC patients. In general, 83% initiate intravenous corticosteroids (IVCS) as initial therapy, whereas 17% initiate infliximab (IFX) (+/-IVCS). At IVCS failure in the vignette, 74% initiated IFX, 15% increased IVCS dose, 7% initiated cyclosporine, and 4% chose colectomy. Of those choosing IFX, 65% chose 5 mg/kg as the initial dose, whereas the remainder chose 10 mg/kg. Twenty-eight percent gave an additional IFX 5 mg/kg and 7% gave an additional 10 mg/kg dose to the patient in the vignette not responding to 5 mg/kg.
Conclusions: Even among experienced inflammatory bowel disease providers, there is significant practice pattern variability in the management of hospitalized UC patients. Future efforts should target this variability. Adjunctively, prospective trials are needed to guide appropriate therapeutic algorithms, especially with respect to positioning and optimally dosing IFX in this population.
Figures
References
-
- Laharie D, Bourreille A, Branche J, et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: a parallel, open-label randomised controlled trial. Lancet. 2012;380:1909–1915. - PubMed
-
- Bernstein C, Ng S, Lakatos P, et al. A review of mortality and surgery in ulcerative colitis: milestones of the seriousness of the disease. Inflamm Bowel Dis. 2013;19:2001–2010. - PubMed
-
- Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2010;105:501–523. quiz 524. - PubMed
-
- Truelove S, Jewell D. Intensive intravenous regimen for severe attacks of ulcerative colitis. Lancet. 1974;1:1067–1070. - PubMed
-
- Jarnerot G, Rolny P, Sandberg-Gertzen H. Intensive intravenous treatment of ulcerative colitis. Gastroenterology. 1985;89:1005–1013. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
