

Acute Kidney Injury Following Exploratory Laparotomy and Temporary Abdominal Closure
- PMID: 28009772
- PMCID: PMC5468485
- DOI: 10.1097/SHK.0000000000000825
Acute Kidney Injury Following Exploratory Laparotomy and Temporary Abdominal Closure
Abstract
Background: Acute kidney injury (AKI) following exploratory laparotomy and temporary abdominal closure (TAC) is poorly understood but clinically significant. We hypothesized that the prevalence of AKI would be highest 96 h following TAC, early hypoxemia would predict AKI, and that AKI would be an independent predictor of mortality.
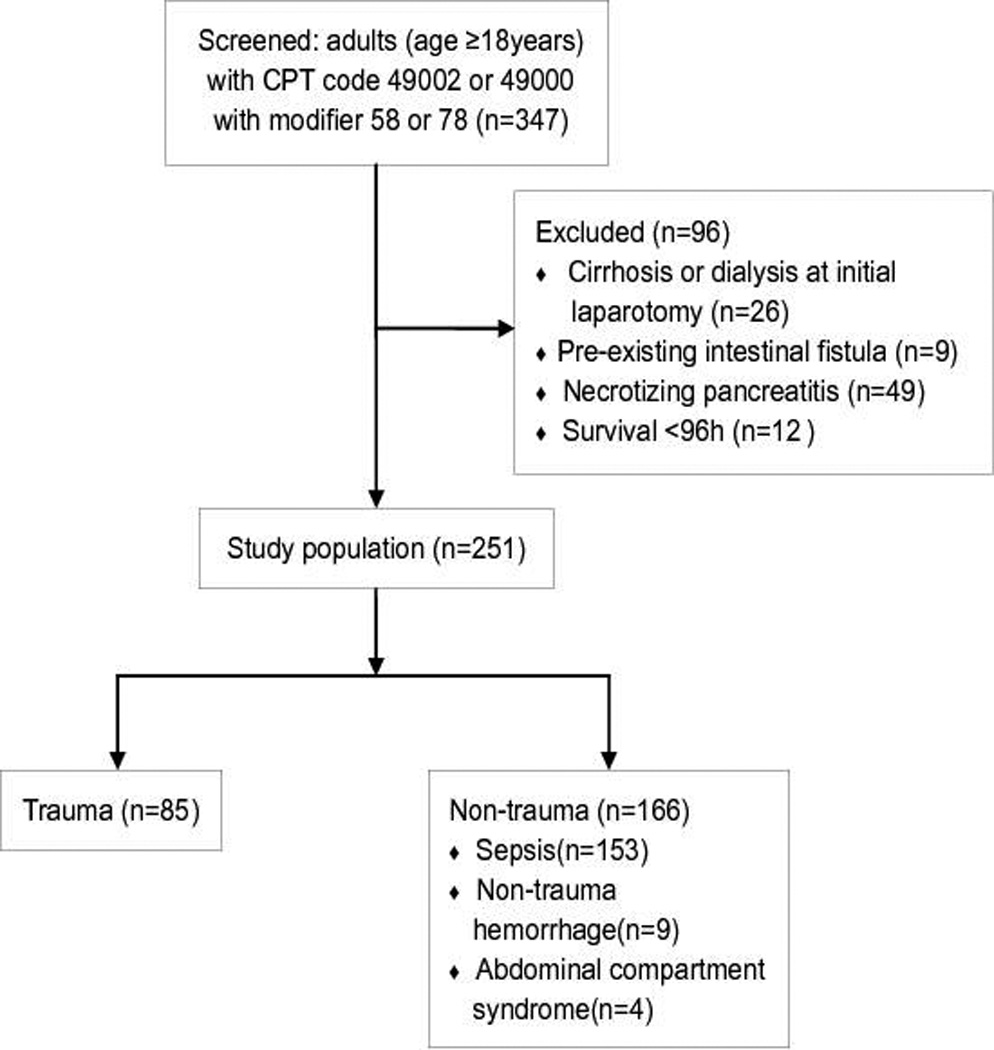
Methods: We performed a retrospective analysis of 251 acute care surgery patients managed with TAC by negative pressure wound therapy (NPWT). Kidney Disease: Improving Global Outcomes AKI stages were assessed on admission, initial TAC, and following TAC at 48 h, 96 h, and 7 d. Multivariate regression was performed to identify risk factors for AKI and inpatient mortality.
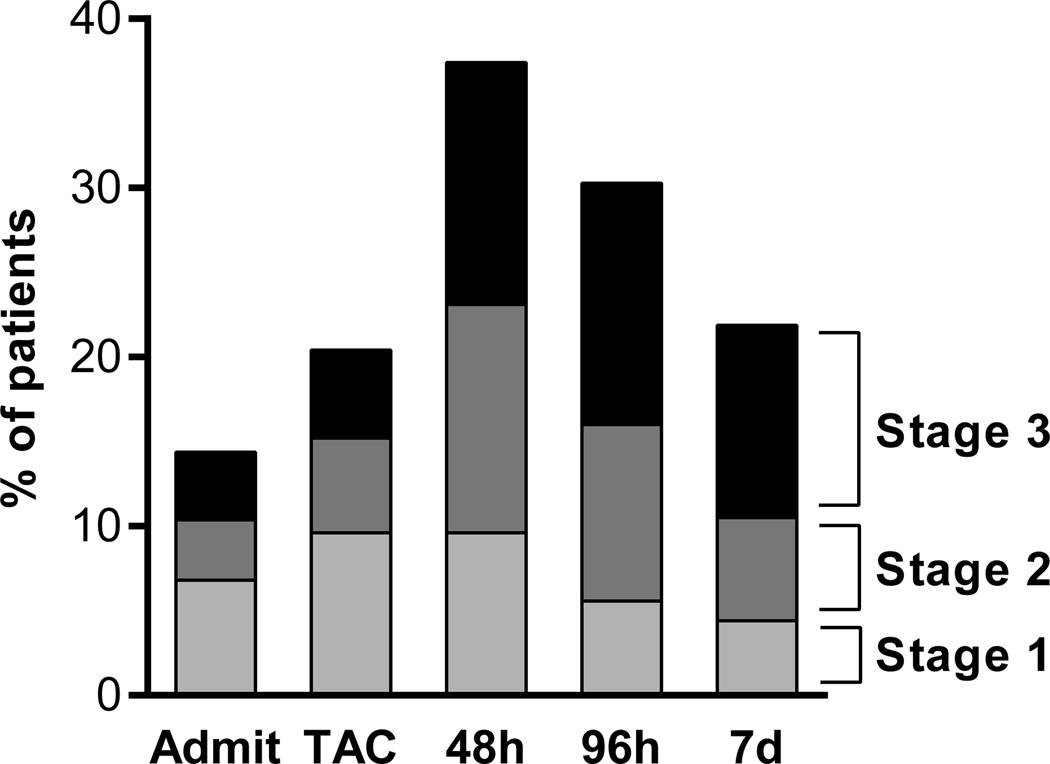
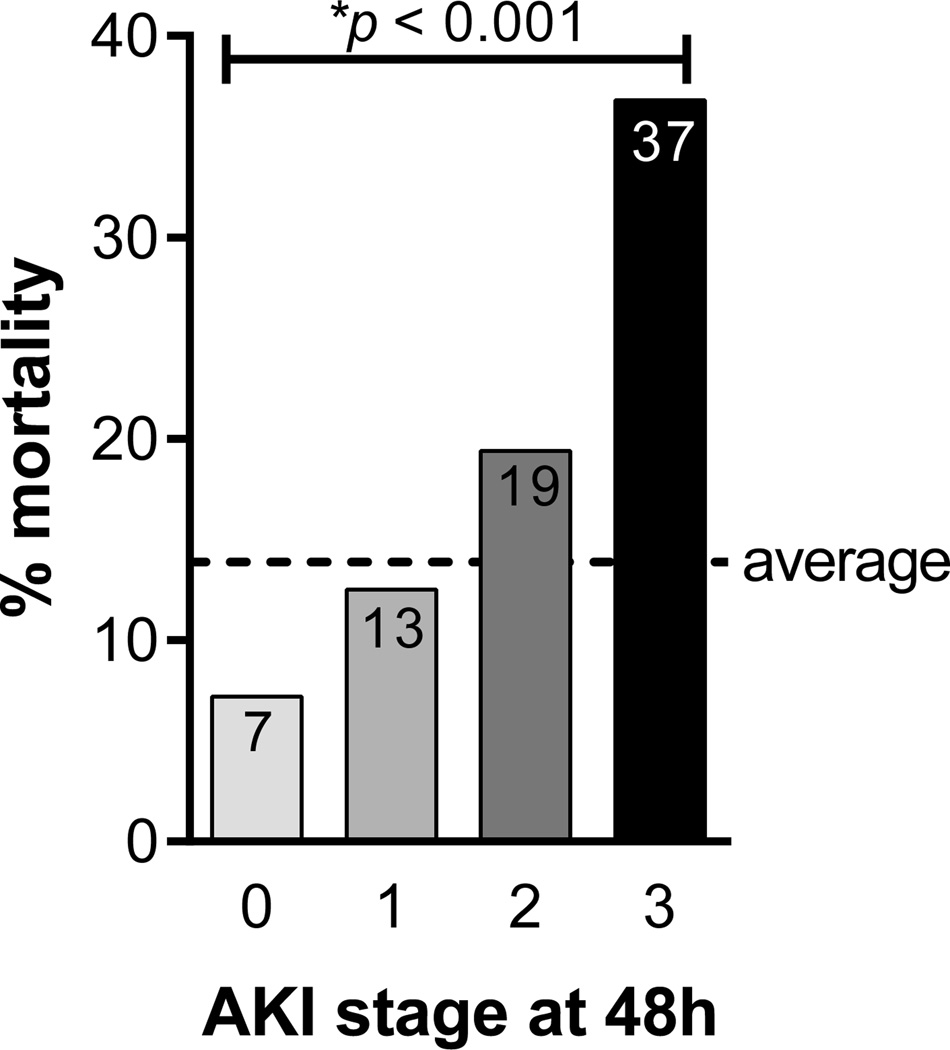
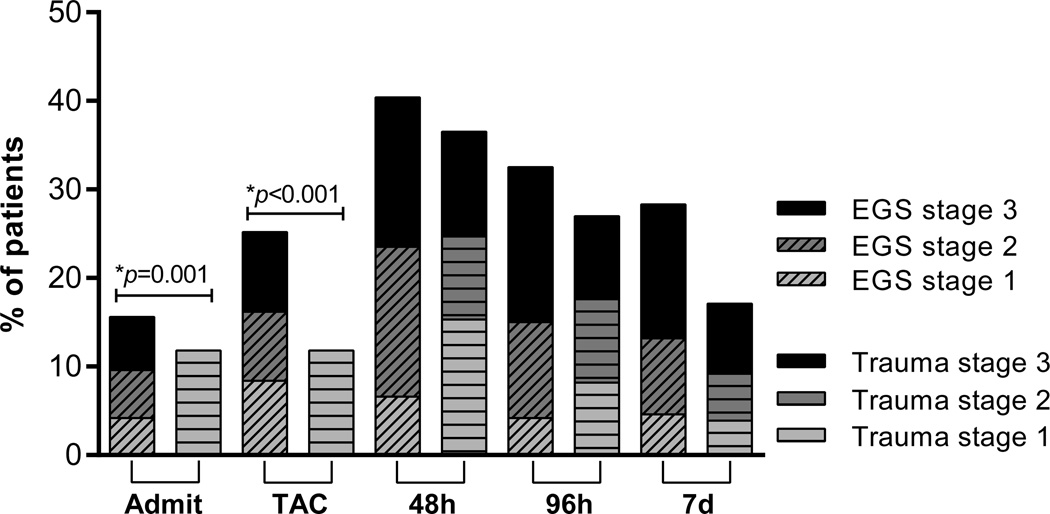
Results: Fifty-seven percent of all patients developed AKI within 7 days of laparotomy (stage 1: 14%, 2: 21%, 3: 22%). The prevalence of AKI peaked 48 h following TAC, and stage correlated with inpatient mortality (stage 0: 7%, 1: 13%, 2: 19%, 3: 37%, P < 0.001). Overall mortality was 14%. Factors predictive of stage 2 or 3 AKI at 48 h included age >65 years (OR 2.6 [95% CI 1.4-4.9]), NPWT output >30 mL/h from first TAC to 48 h (2.0 [1.1-3.9]), and three parameters at initial laparotomy: mean arterial pressure <60 mm Hg (2.9 [1.0-8.5]), temperature <36°C (2.1 [1.1-3.8]), and anion gap >21 mEq/L (1.9 [1.0-3.7]). AKI was an independent predictor of inpatient mortality (5.5 [2.5-11.8]).
Conclusions: AKI is common following TAC, reaches greatest prevalence 48 h after initial laparotomy, and is associated with increased mortality. NPWT fluid loss is a risk factor for AKI that is unique to TAC patients.
Conflict of interest statement
The authors have no relevant conflicts of interest.
Figures
References
-
- Rotondo MF, Schwab CW, McGonigal MD, Phillips GR, 3rd, Fruchterman TM, Kauder DR, Latenser BA, Angood PA. 'Damage control': an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma. 1993;35(3):375–382. discussion 382-3. - PubMed
-
- Diaz JJ, Jr, Cullinane DC, Dutton WD, Jerome R, Bagdonas R, Bilaniuk JW, Collier BR, Como JJ, Cumming J, Griffen M, et al. The management of the open abdomen in trauma and emergency general surgery: part 1-damage control. J Trauma. 2010;68(6):1425–1438. - PubMed
-
- Moore EE, Thomas G. Orr Memorial Lecture. Staged laparotomy for the hypothermia, acidosis, and coagulopathy syndrome. Am J Surg. 1996;172(5):405–410. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
