

Kidney Transplant With Low Levels of DSA or Low Positive B-Flow Crossmatch: An Underappreciated Option for Highly Sensitized Transplant Candidates
- PMID: 28009780
- PMCID: PMC5481511
- DOI: 10.1097/TP.0000000000001619
Kidney Transplant With Low Levels of DSA or Low Positive B-Flow Crossmatch: An Underappreciated Option for Highly Sensitized Transplant Candidates
Abstract
Background: Avoiding donor-specific antibody (DSA) is difficult for sensitized patients. Improved understanding of the risk of low level DSA is needed.
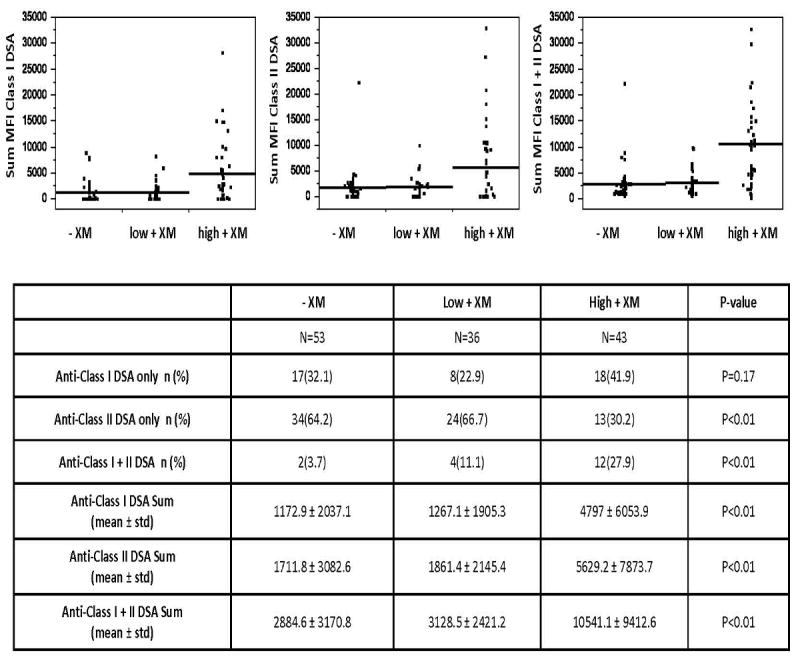
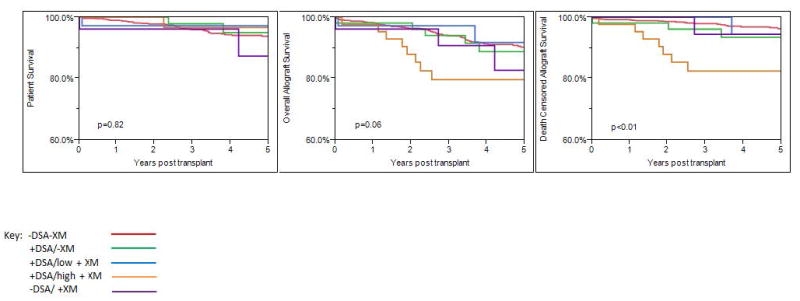
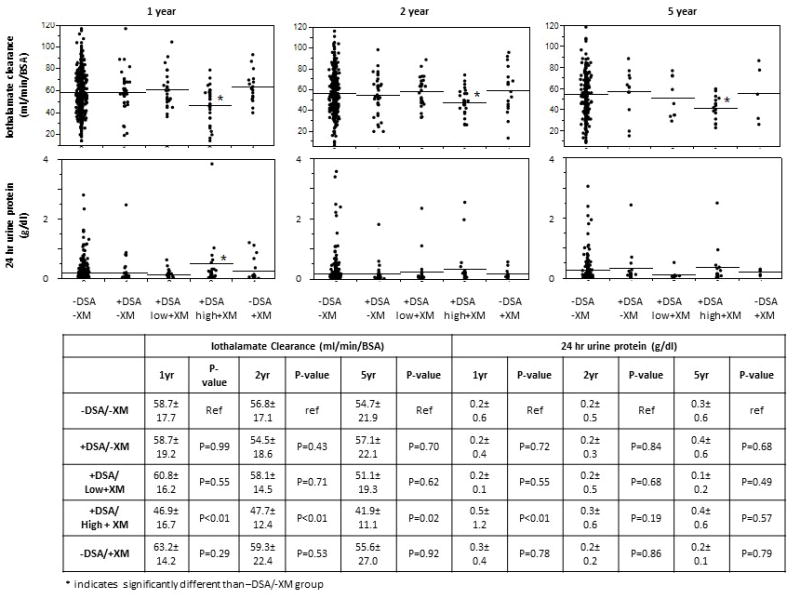
Methods: We retrospectively compared the outcomes of 954 patients transplanted with varied levels of baseline DSA detected by single antigen beads and B flow cytometric crossmatch (XM). Patients were grouped as follows: -DSA/-XM, +DSA/-XM, +DSA/low +XM, +DSA/high +XM, and -DSA/+XM and followed up for a mean of 4.1 ± 1.9 years (similar among groups, P = 0.49).
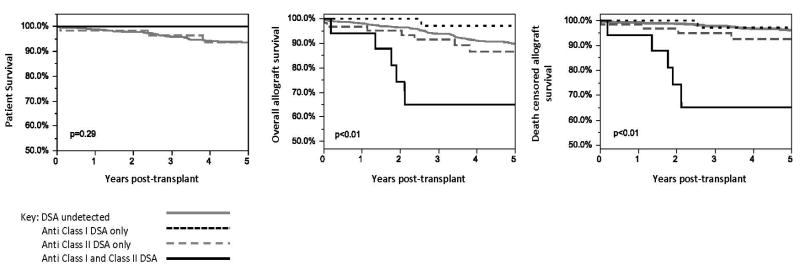
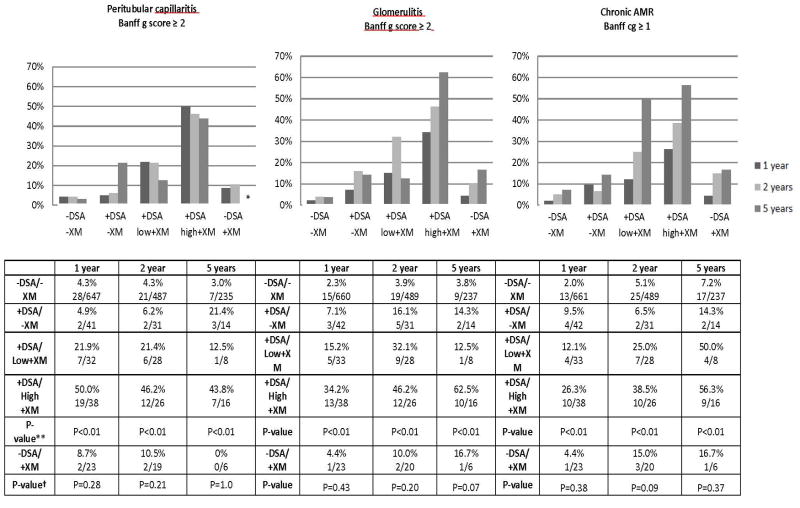
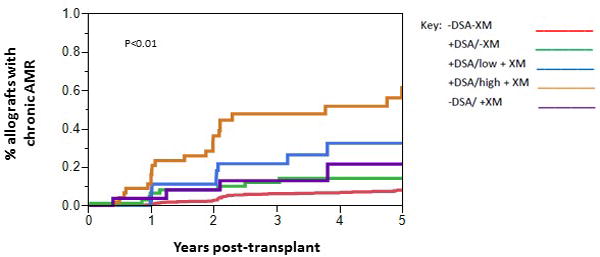
Results: Death-censored allograft survival was similar in all groups except the +DSA/high +XM group, which was lower at 79.1% versus 96.2% in the -DSA/-XM group (P < 0.01). The incidence of chronic antibody-mediated rejection (CAMR) based on surveillance biopsy was higher with increasing DSA (8.2% -DSA/-XM, 17.0% +DSA/-XM, 30.6% +DSA/low +XM, and 51.2% +DSA/high +XM, P < 0.01), but similar in groups without baseline DSA (8.1% -DSA/-XM vs 15.4% -DSA/+XM, P = 0.19). Having a calculated panel-reactive antibody (cPRA) of 80% or greater was independently associated with CAMR (hazard ratio, 5.2; P = 0.03) even when DSA was undetected at baseline. By 2 years posttransplant, the incidence of CAMR was 19.4% in patients with cPRA of 80% or greater and undetected DSA and negative XM at baseline.
Conclusions: Kidney transplantation with low-level DSA with or without a low positive XM is a reasonable option for highly sensitized patients and may be advantageous compared with waiting for a negative XM deceased donor. The risk for CAMR is low in patients with no DSA even if the XM is positive. Patients with cPRA of 80% or greater are at risk for CAMR even if no DSA is detected.
Conflict of interest statement
Participated in research design;
Participated in the writing of the paper
Participated in the data collection
Participated in data analysis
Schinstock declares conflict of interest: Alexion Pharmaceuticals
Participated in research design
Participated in the writing of the paper
Participated in data analysis
Gandhi declares no conflict of interest
Participated in the writing of the paper
Participated in the data collection
Participated in data analysis
Cheungpasitporn declares no conflict of interest
Participated in the writing of the paper
Participated in the data collection
Participated in data analysis
Mitema declares no conflict of interest
Participated in the writing of the paper
Participated in data analysis
Prieto declares no conflict of interest
Participated in the writing of the paper
Participated in data analysis
Dean declares no conflict of interest
Participated in the writing of the paper
Participated in the data collection
Participated in data analysis
Cornell declares conflict of interest: Alexion Pharmaceuticals
Participated in the writing of the paper
Participated in data analysis
Participated in design of research
Cosio declares no conflict of interest
Participated in the design of the research
Participated in data analysis
Participated in the writing of the paper
Stegall declares conflict of interest: Alexion Pharmaceuticals
Figures
References
-
- Gloor JM, Cosio FG, Rea DJ, et al. Histologic findings one year after positive crossmatch or ABO blood group incompatible living donor kidney transplantation. Am J Transplant. 2006;6(8):1841–1847. - PubMed
-
- Loupy A, Suberbielle-Boissel C, Hill GS, et al. Outcome of subclinical antibody-mediated rejection in kidney transplant recipients with preformed donor-specific antibodies. Am J Transplant. 2009;9(11):2561–2570. - PubMed
-
- Glotz D, Antoine C, Julia P, et al. Desensitization and subsequent kidney transplantation of patients using intravenous immunoglobulins (IVIg) Am J Transplant. 2002;2(8):758–760. - PubMed
-
- Bentall A, Cornell LD, Gloor JM, et al. Five-year outcomes in living donor kidney transplants with a positive crossmatch. Am J Transplant. 2013;13(1):76–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
