

Refractory status epilepticus in children with and without prior epilepsy or status epilepticus
- PMID: 28011930
- PMCID: PMC5272971
- DOI: 10.1212/WNL.0000000000003550
Refractory status epilepticus in children with and without prior epilepsy or status epilepticus
Abstract
Objective: To compare refractory convulsive status epilepticus (rSE) management and outcome in children with and without a prior diagnosis of epilepsy and with and without a history of status epilepticus (SE).
Methods: This was a prospective observational descriptive study performed from June 2011 to May 2016 on pediatric patients (1 month-21 years of age) with rSE.
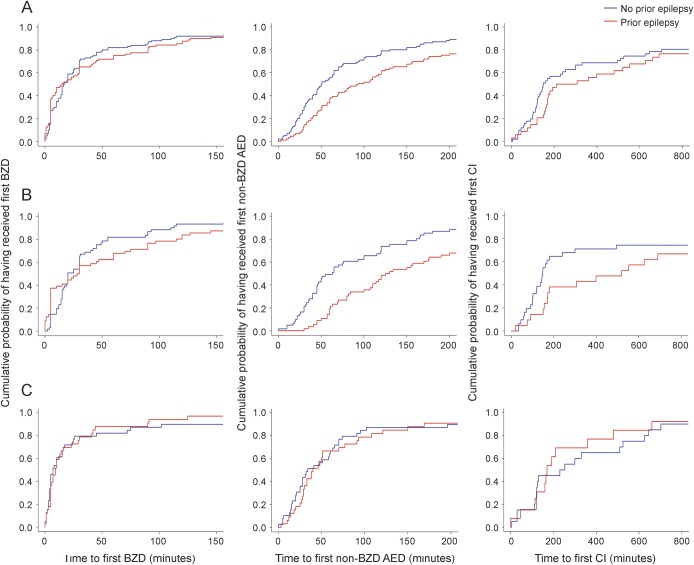
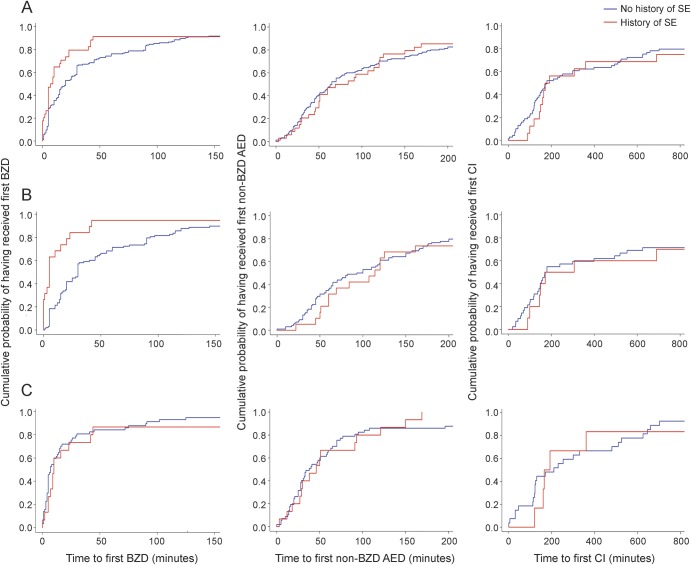
Results: We enrolled 189 participants (53% male) with a median (25th-75th percentile) age of 4.2 (1.3-9.6) years. Eighty-nine (47%) patients had a prior diagnosis of epilepsy. Thirty-four (18%) patients had a history of SE. The time to the first benzodiazepine was similar in participants with and without a diagnosis of epilepsy (15 [5-60] vs 16.5 [5-42.75] minutes, p = 0.858). Patients with a diagnosis of epilepsy received their first non-benzodiazepine (BZD) antiepileptic drug (AED) later (93 [46-190] vs 50.5 [28-116] minutes, p = 0.002) and were less likely to receive at least one continuous infusion (35/89 [39.3%] vs 57/100 [57%], p = 0.03). Compared to patients with no history of SE, patients with a history of SE received their first BZD earlier (8 [3.5-22.3] vs 20 [5-60] minutes, p = 0.0073), although they had a similar time to first non-BZD AED (76.5 [45.3-124] vs 65 [32.5-156] minutes, p = 0.749). Differences were mostly driven by the patients with an out-of-hospital rSE onset.
Conclusions: Our study establishes that children with rSE do not receive more timely treatment if they have a prior diagnosis of epilepsy; however, a history of SE is associated with more timely administration of abortive medication.
© 2016 American Academy of Neurology.
Figures
References
-
- Chin RF, Neville BG, Peckham C, et al. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: prospective population-based study. Lancet 2006;368:222–229. - PubMed
-
- Dham BS, Hunter K, Rincon F. The epidemiology of status epilepticus in the United States. Neurocrit Care 2014;20:476–483. - PubMed
-
- Hesdorffer DC, Logroscino G, Cascino G, Annegers JF, Hauser WA. Incidence of status epilepticus in Rochester, Minnesota, 1965-1984. Neurology 1998;50:735–741. - PubMed
-
- Penberthy LT, Towne A, Garnett LK, Perlin JB, DeLorenzo RJ. Estimating the economic burden of status epilepticus to the health care system. Seizure 2005;14:46–51. - PubMed
-
- Strzelczyk A, Knake S, Oertel WH, Rosenow F, Hamer HM. Inpatient treatment costs of status epilepticus in adults in Germany. Seizure 2013;22:882–885. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases