

Ankle-brachial index and physical function in older individuals: The Atherosclerosis Risk in Communities (ARIC) study
- PMID: 28012644
- PMCID: PMC5325783
- DOI: 10.1016/j.atherosclerosis.2016.11.023
Ankle-brachial index and physical function in older individuals: The Atherosclerosis Risk in Communities (ARIC) study
Abstract
Background and aims: Most prior studies investigating the association of lower extremity peripheral artery disease (PAD) with physical function were small or analyzed selected populations (e.g., patients at vascular clinics or persons with reduced function), leaving particular uncertainty regarding the association in the general community.
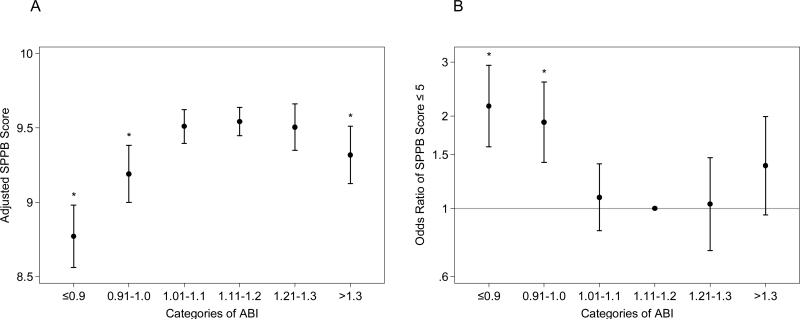
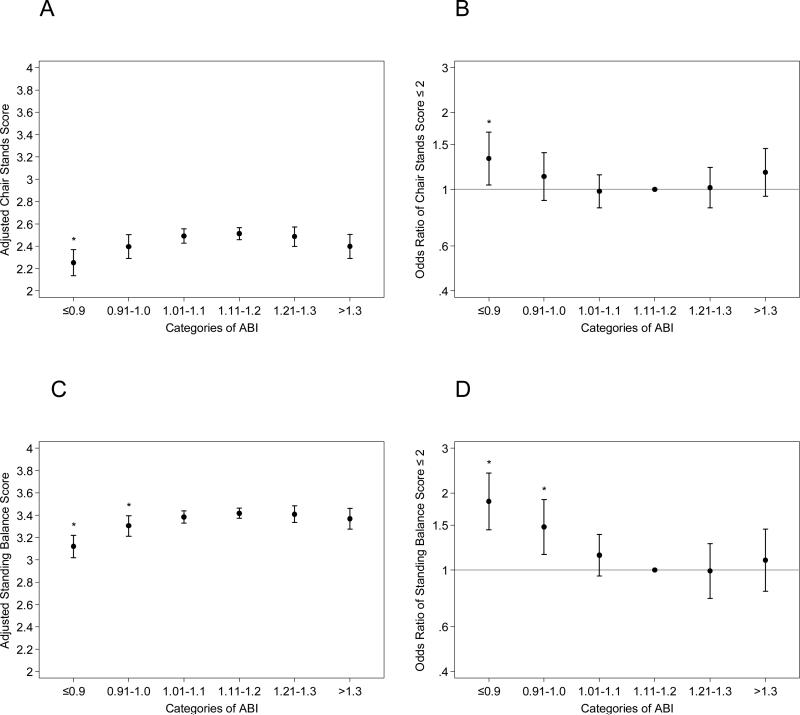
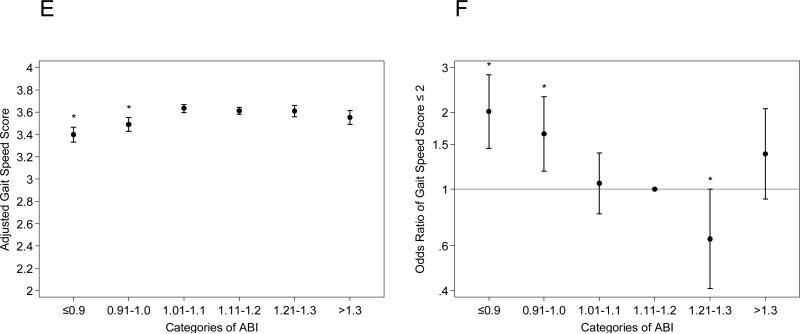
Methods: Among 5262 ARIC participants (age 71-90 years during 2011-2013), we assessed the cross-sectional association of ankle-brachial index (ABI) with the Short Physical Performance Battery (SPPB) score (0-12), its individual components (chair stands, standing balance, and gait speed) (0-4 points each), and grip strength after accounting for potential confounders, including a history of coronary disease, stroke, or heart failure.
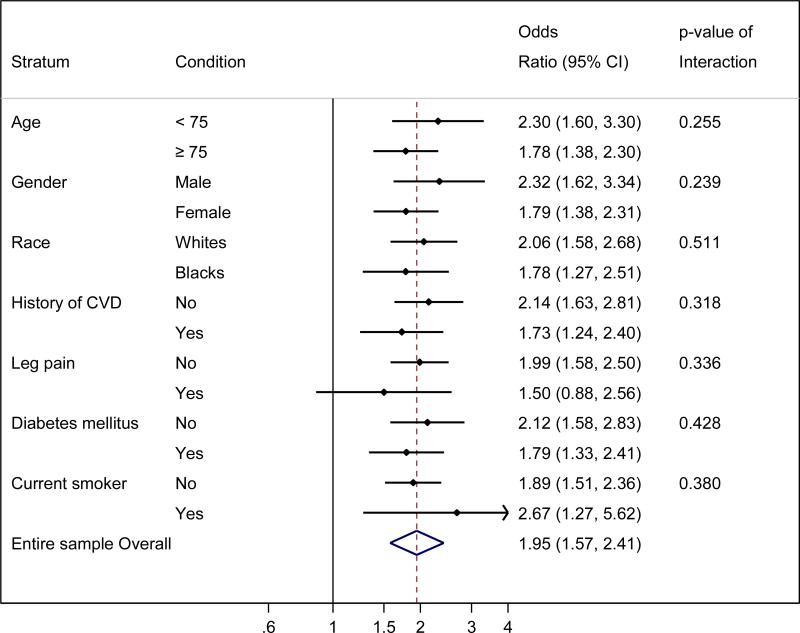
Results: There were 411 participants (7.8%) with low ABI ≤0.90 and 469 (8.9%) participants with borderline low ABI 0.91-1.00. Both ABI ≤0.90 and 0.91-1.00 were independently associated with poor physical function (SPPB score ≤6) compared to ABI 1.11-1.20 (adjusted odds ratio 2.10 [95% CI 1.55-2.84] and 1.86 [1.38-2.51], respectively). The patterns were largely consistent across subgroups by clinical conditions (e.g., leg pain or other cardiovascular diseases), in every SPPB component, and for grip strength. ABI >1.3 (472 participants [9.0%]), indicative of non-compressible pedal arteries, was related to lower physical function as well but did not necessarily reach significance.
Conclusions: In community-dwelling older adults, low and borderline low ABI suggestive of PAD were independently associated with poorer systemic physical function compared to those with normal ABI. Clinical attention to PAD as a potential contributor to poor physical function is warranted in community-dwelling older adults.
Keywords: Aging; Peripheral artery disease; Physical function.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Figures
Comment in
-
Peripheral arterial disease and loss of physical function: Just two old friends?Atherosclerosis. 2017 Feb;257:246-247. doi: 10.1016/j.atherosclerosis.2016.12.015. Epub 2016 Dec 15. Atherosclerosis. 2017. PMID: 28038769 No abstract available.
References
-
- Hirsch AT, Duval S. The global pandemic of peripheral artery disease. Lancet. 2013;382:1312–1314. - PubMed
-
- Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UKA, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. The Lancet. 2013;382:1329–1340. - PubMed
-
- Varu VN, Hogg ME, Kibbe MR. Critical limb ischemia. Journal of Vascular Surgery. 2010;51:230–241. - PubMed
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation. 2004;110:738–743. - PubMed
-
- Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, McCann TJ, Browner D. Mortality over a period of 10 years in patients with peripheral arterial disease. The New England journal of medicine. 1992;326:381–386. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- T32 HL007055/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- R01 AG053938/AG/NIA NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- K24 DK106414/DK/NIDDK NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
