

Myocardial Fibrosis and Cardiac Decompensation in Aortic Stenosis
- PMID: 28017384
- PMCID: PMC5683736
- DOI: 10.1016/j.jcmg.2016.10.007
Myocardial Fibrosis and Cardiac Decompensation in Aortic Stenosis
Abstract
Objectives: Cardiac magnetic resonance (CMR) was used to investigate the extracellular compartment and myocardial fibrosis in patients with aortic stenosis, as well as their association with other measures of left ventricular decompensation and mortality.
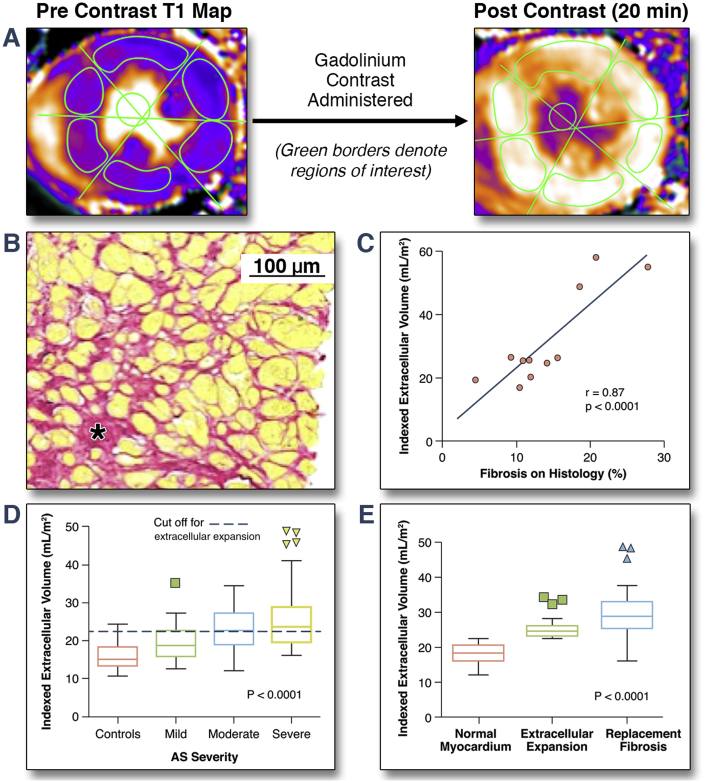
Background: Progressive myocardial fibrosis drives the transition from hypertrophy to heart failure in aortic stenosis. Diffuse fibrosis is associated with extracellular volume expansion that is detectable by T1 mapping, whereas late gadolinium enhancement (LGE) detects replacement fibrosis.
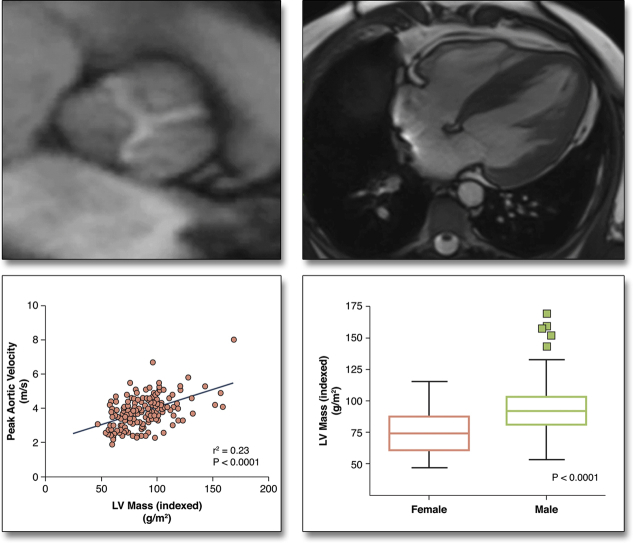
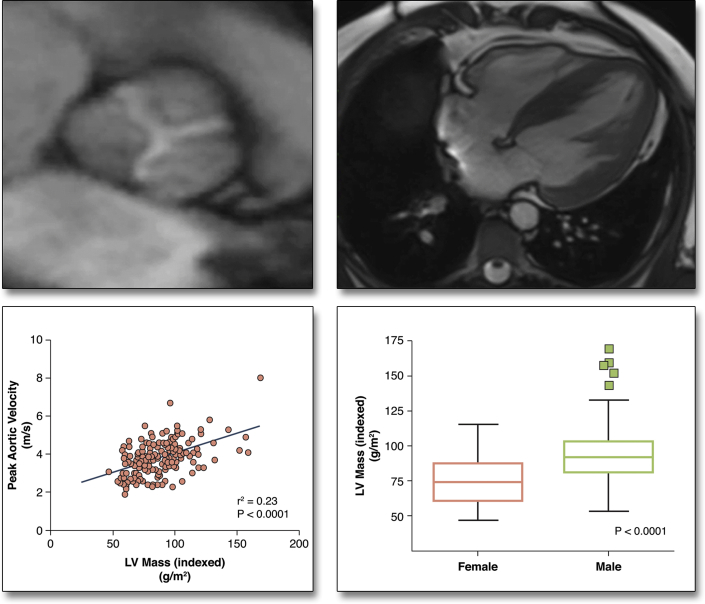
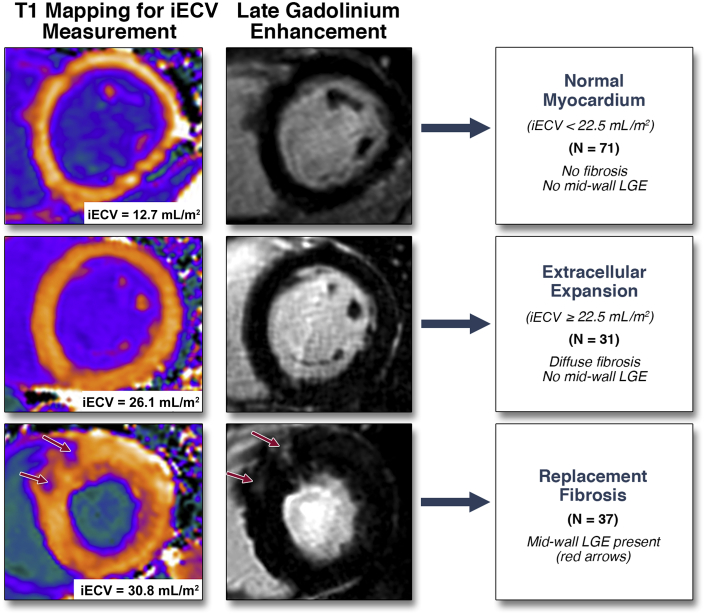
Methods: In a prospective observational cohort study, 203 subjects (166 with aortic stenosis [69 years; 69% male]; 37 healthy volunteers [68 years; 65% male]) underwent comprehensive phenotypic characterization with clinical imaging and biomarker evaluation. On CMR, we quantified the total extracellular volume of the myocardium indexed to body surface area (iECV). The iECV upper limit of normal from the control group (22.5 ml/m2) was used to define extracellular compartment expansion. Areas of replacement mid-wall LGE were also identified. All-cause mortality was determined during 2.9 ± 0.8 years of follow up.
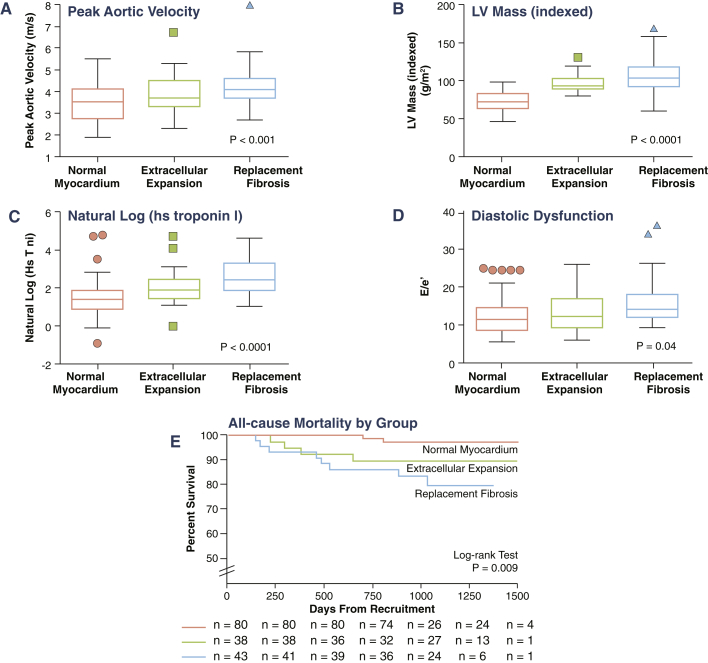
Results: iECV demonstrated a good correlation with diffuse histological fibrosis on myocardial biopsies (r = 0.87; p < 0.001; n = 11) and was increased in patients with aortic stenosis (23.6 ± 7.2 ml/m2 vs. 16.1 ± 3.2 ml/m2 in control subjects; p < 0.001). iECV was used together with LGE to categorize patients with normal myocardium (iECV <22.5 ml/m2; 51% of patients), extracellular expansion (iECV ≥22.5 ml/m2; 22%), and replacement fibrosis (presence of mid-wall LGE, 27%). There was evidence of increasing hypertrophy, myocardial injury, diastolic dysfunction, and longitudinal systolic dysfunction consistent with progressive left ventricular decompensation (all p < 0.05) across these groups. Moreover, this categorization was of prognostic value with stepwise increases in unadjusted all-cause mortality (8 deaths/1,000 patient-years vs. 36 deaths/1,000 patient-years vs. 71 deaths/1,000 patient-years, respectively; p = 0.009).
Conclusions: CMR detects ventricular decompensation in aortic stenosis through the identification of myocardial extracellular expansion and replacement fibrosis. This holds major promise in tracking myocardial health in valve disease and for optimizing the timing of valve replacement. (The Role of Myocardial Fibrosis in Patients With Aortic Stenosis; NCT01755936).
Keywords: T1 mapping; aortic stenosis; fibrosis; hypertrophy; magnetic resonance imaging; myocardium.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Myocardial Fibrosis in Aortic Stenosis.JACC Cardiovasc Imaging. 2017 Nov;10(11):1334-1336. doi: 10.1016/j.jcmg.2016.09.022. Epub 2016 Dec 21. JACC Cardiovasc Imaging. 2017. PMID: 28017392 No abstract available.
-
ECV for Patients With Aortic Stenosis: Which Patient Will Benefit?JACC Cardiovasc Imaging. 2017 Nov;10(11):1408-1409. doi: 10.1016/j.jcmg.2017.10.003. JACC Cardiovasc Imaging. 2017. PMID: 29122141 No abstract available.
References
-
- Nkomo V.T., Gardin J.M., Skelton T.N., Gottdiener J.S., Scott C.G., Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Dweck M.R., Boon N.A., Newby D.E. Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol. 2012;60:1854–1863. - PubMed
-
- Hein S., Arnon E., Kostin S. Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation. 2003;107:984–991. - PubMed
-
- Flett A.S., Hayward M.P., Ashworth M.T. Equilibrium contrast cardiovascular magnetic resonance for the measurement of diffuse myocardial fibrosis: preliminary validation in humans. Circulation. 2010;122:138–144. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
