

Ex Vivo CD34+-Selected T Cell-Depleted Peripheral Blood Stem Cell Grafts for Allogeneic Hematopoietic Stem Cell Transplantation in Acute Leukemia and Myelodysplastic Syndrome Is Associated with Low Incidence of Acute and Chronic Graft-versus-Host Disease and High Treatment Response
- PMID: 28017734
- PMCID: PMC5398850
- DOI: 10.1016/j.bbmt.2016.12.633
Ex Vivo CD34+-Selected T Cell-Depleted Peripheral Blood Stem Cell Grafts for Allogeneic Hematopoietic Stem Cell Transplantation in Acute Leukemia and Myelodysplastic Syndrome Is Associated with Low Incidence of Acute and Chronic Graft-versus-Host Disease and High Treatment Response
Abstract
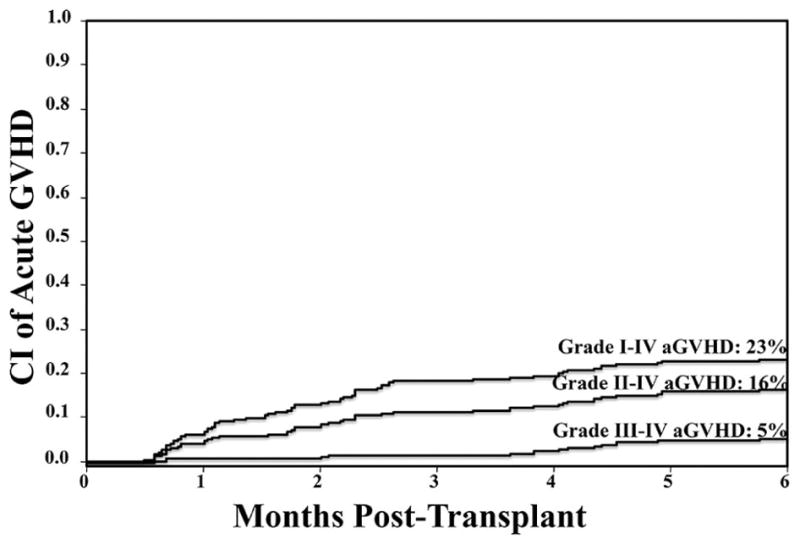
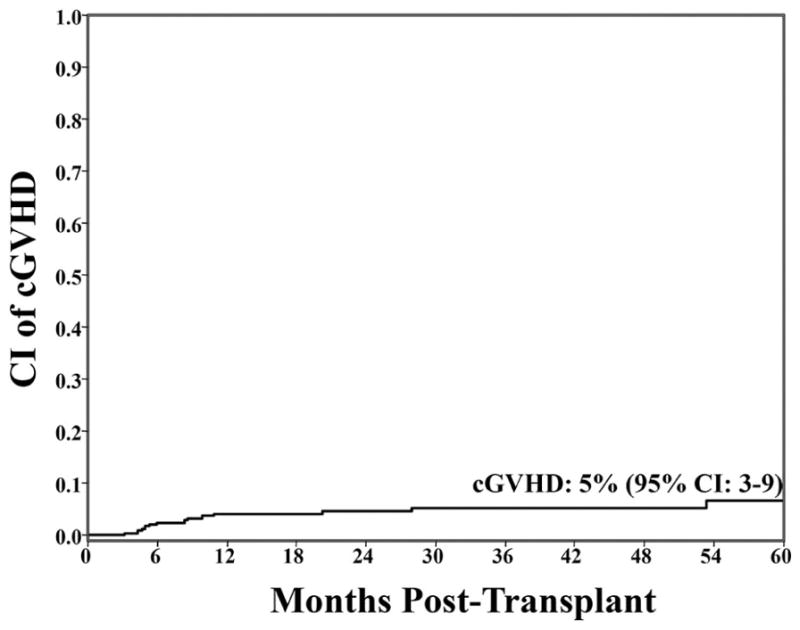
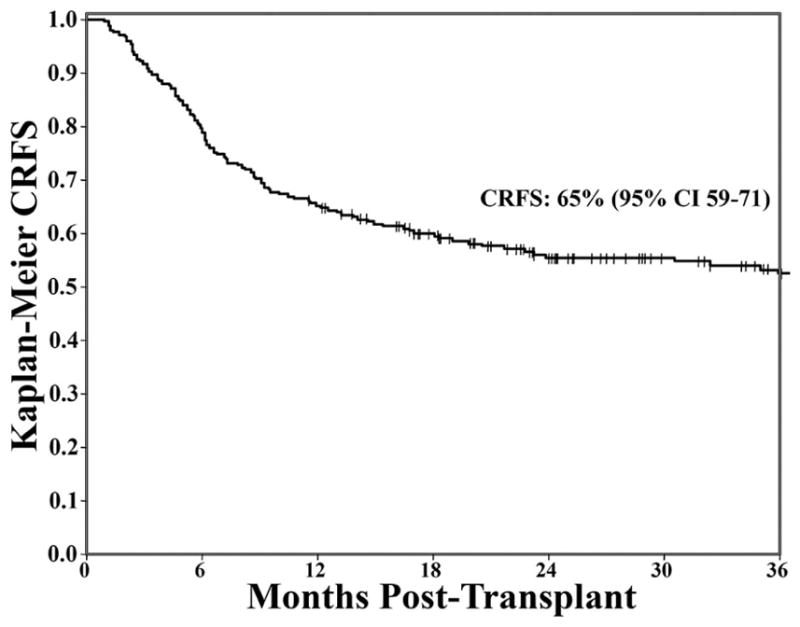
Ex vivo CD34+-selected T cell depletion (TCD) has been developed as a strategy to reduce the incidence of graft-versus-host disease (GVHD) after allogeneic (allo) hematopoietic stem cell transplantation (HSCT). Clinical characteristics, treatment responses, and outcomes of patients developing acute (aGVHD) and chronic GVHD (cGVHD) after TCD allo-HSCT have not been well established. We evaluated 241 consecutive patients (median age, 57 years) with acute leukemia (n = 191, 79%) or myelodysplastic syndrome (MDS) (n = 50, 21%) undergoing CD34+-selected TCD allo-HSCT without post-HCST immunosuppression in a single institution. Cumulative incidences of grades II-IV and III-IV aGVHD at 180 days were 16% (95% confidence interval [CI], 12 to 21) and 5% (95% CI, 3 to 9), respectively. The skin was the most frequent organ involved, followed by the gastrointestinal tract. Patients were treated with topical corticosteroids, poorly absorbed corticosteroids (budesonide), and/or systemic corticosteroids. The overall day 28 treatment response was high at 82%. The cumulative incidence of any cGVHD at 3 years was 5% (95% CI, 3 to 9), with a median time of onset of 256 days (range, 95 to 1645). The 3-year transplant-related mortality, relapse, overall survival, and disease-free survival were 24% (95% CI, 18 to 30), 22% (95% CI, 17 to 27), 57% (95% CI, 50 to 64), and 54% (95% CI, 47 to 61), respectively. The 1-year and 3-year probabilities of cGVHD-free/relapse-free survival were 65% (95% CI, 59 to 71) and 52% (95% CI, 45 to 59), respectively. Our findings support the use of ex vivo CD34+-selected TCD allograft as a calcineurin inhibitor-free intervention for the prevention of GVHD in patients with acute leukemia and MDS.
Keywords: Acute graft-versus-host disease; Chronic graft-versus-host disease; T cell–depleted transplantation.
Copyright © 2017 The American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Nash RA, Antin JH, Karanes C, et al. Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood. 2000;96(6):2062–2068. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
