

Management of neuroendocrine carcinomas of the pancreas (WHO G3): A tailored approach between proliferation and morphology
- PMID: 28018101
- PMCID: PMC5143761
- DOI: 10.3748/wjg.v22.i45.9944
Management of neuroendocrine carcinomas of the pancreas (WHO G3): A tailored approach between proliferation and morphology
Abstract
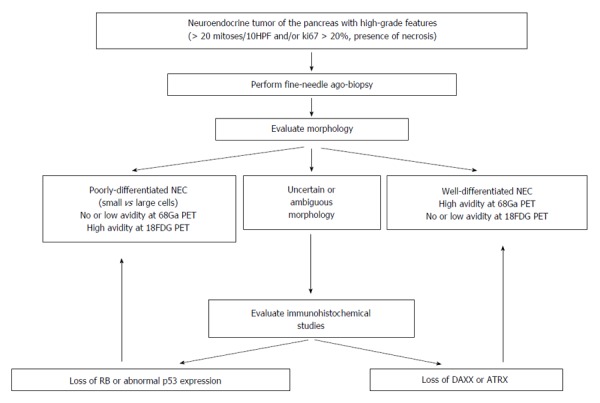
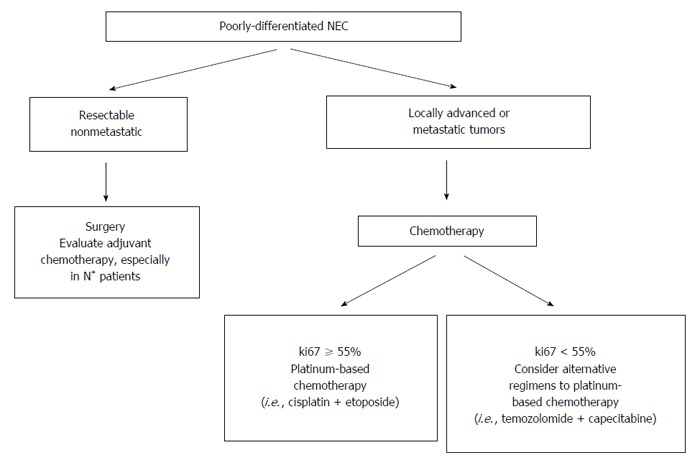
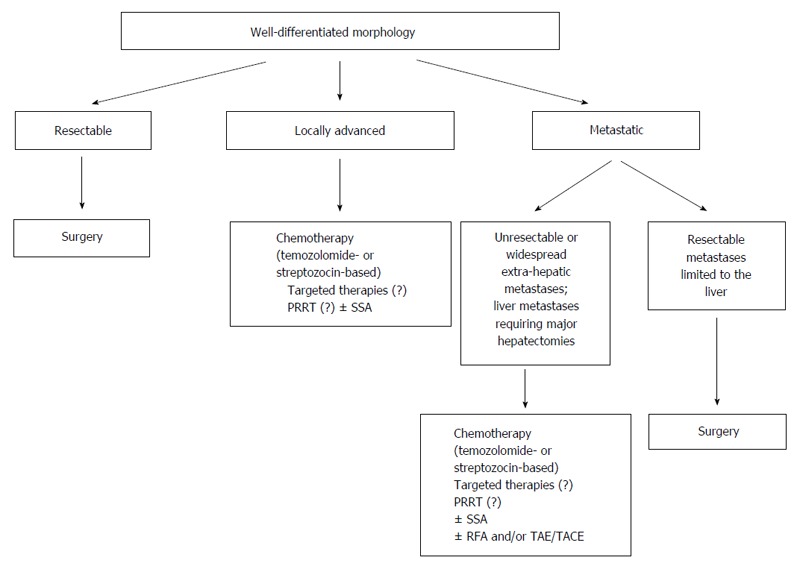
Neuroendocrine carcinomas (NEC) of the pancreas are defined by a mitotic count > 20 mitoses/10 high power fields and/or Ki67 index > 20%, and included all the tumors previously classified as poorly differentiated endocrine carcinomas. These latter are aggressive malignancies with a high propensity for distant metastases and poor prognosis, and they can be further divided into small- and large-cell subtypes. However in the NEC category are included also neuroendocrine tumors with a well differentiated morphology but ki67 index > 20%. This category is associated with better prognosis and does not significantly respond to cisplatin-based chemotherapy, which represents the gold standard therapeutic approach for poorly differentiated NEC. In this review, the differences between well differentiated and poorly differentiated NEC are discussed considering both pathology, imaging features, treatment and prognostic implications. Diagnostic and therapeutic flowcharts are proposed. The need for a revision of current classification system is stressed being well differentiated NEC a more indolent disease compared to poorly differentiated tumors.
Keywords: Chemotherapy; Metastases; Morphology; Neuroendocrine carcinomas; Pancreatic neuroendocrine tumors; Prognosis; Proliferation; Surgery.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest, no financial support.
Figures
References
-
- Solcia E, Capella C, Kloppel G, Heitz PU, Sobin LH, Rosai J. Endocrine tumours of the gastrointestinal tract. In: Solcia E, Kloppel G and Sobin LH, editors. Histologic typing of endocrine tumours, WHO international histological classification of tumours. New York: Springer Verlag; 2000. pp. 57–67.
-
- Rindi G, Arnold R, Bosman FT. Nomenclature and classification of neuroendocrine neoplasms of the digestive system. In Bosman FT, Carneiro F, Hruban RH and Theise ND. WHO Classification of Tumors of the Digestive System. Lyon: IARC Press; 2010. pp. 13–14.
-
- Crippa S, Partelli S, Boninsegna L, Falconi M. Implications of the new histological classification (WHO 2010) for pancreatic neuroendocrine neoplasms. Ann Oncol. 2012;23:1928. - PubMed
-
- Garcia-Carbonero R, Sorbye H, Baudin E, Raymond E, Wiedenmann B, Niederle B, Sedlackova E, Toumpanakis C, Anlauf M, Cwikla JB, et al. ENETS Consensus Guidelines for High-Grade Gastroenteropancreatic Neuroendocrine Tumors and Neuroendocrine Carcinomas. Neuroendocrinology. 2016;103:186–194. - PubMed
-
- Sorbye H, Strosberg J, Baudin E, Klimstra DS, Yao JC. Gastroenteropancreatic high-grade neuroendocrine carcinoma. Cancer. 2014;120:2814–2823. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
