

Preoperative evaluation of pancreatic ductal adenocarcinoma with synchronous liver metastasis: Diagnosis and assessment of unresectability
- PMID: 28018110
- PMCID: PMC5143749
- DOI: 10.3748/wjg.v22.i45.10024
Preoperative evaluation of pancreatic ductal adenocarcinoma with synchronous liver metastasis: Diagnosis and assessment of unresectability
Abstract
Aim: To identify predictors for synchronous liver metastasis from resectable pancreatic ductal adenocarcinoma (PDAC) and assess unresectability of synchronous liver metastasis.
Methods: Retrospective records of PDAC patients with synchronous liver metastasis who underwent simultaneous resections of primary PDAC and synchronous liver metastasis, or palliative surgical bypass, were collected from 2007 to 2015. A series of pre-operative clinical parameters, including tumor markers and inflammation-based indices, were analyzed by logistic regression to figure out predictive factors and assess unresectability of synchronous liver metastasis. Cox regression was used to identify prognostic factors in liver-metastasized PDAC patients after surgery, with intention to validate their conformance to the indications of simultaneous resections and palliative surgical bypass. Survival of patients from different groups were analyzed by the Kaplan-Meier method. Intra- and post-operative courses were compared, including complications. PDAC patients with no distant metastases who underwent curative resection served as the control group.
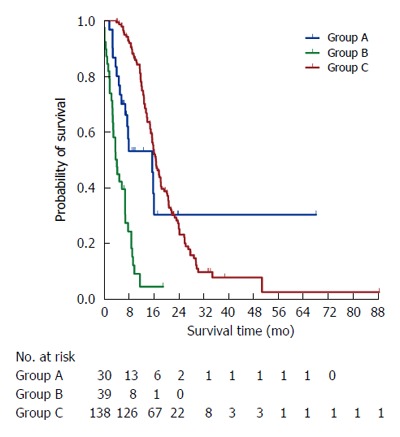
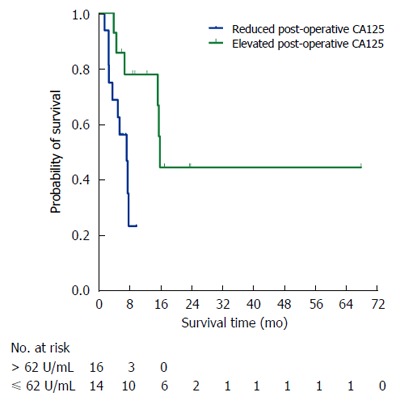
Results: CA125 > 38 U/mL (OR = 12.397, 95%CI: 5.468-28.105, P < 0.001) and diabetes mellitus (OR = 3.343, 95%CI: 1.539-7.262, P = 0.002) independently predicted synchronous liver metastasis from resectable PDAC. CA125 > 62 U/mL (OR = 5.181, 95%CI: 1.612-16.665, P = 0.006) and age > 62 years (OR = 3.921, 95%CI: 1.217-12.632, P = 0.022) correlated with unresectability of synchronous liver metastasis, both of which also indicated a worse long-term outcome of liver-metastasized PDAC patients after surgery. After the simultaneous resections, patients with post-operatively elevated serum CA125 levels had shorter survival than those with post-operatively reduced serum CA125 levels (7.7 mo vs 16.3 mo, P = 0.013). The survival of liver-metastasized PDAC patients who underwent the simultaneous resections was similar to that of non-metastasized PDAC patients who underwent curative pancreatectomy alone (7.0 mo vs 16.9 mo, P < 0.001), with no higher rates of either pancreatic fistula (P = 0.072) or other complications (P = 0.230) and no greater impacts on length of hospital stay (P = 0.602) or post-operative diabetic control (P = 0.479).
Conclusion: The criterion set up by CA125 levels could facilitate careful diagnosis of synchronous liver metastases from PDAC, and prudent selection of appropriate patients for the simultaneous resections.
Keywords: CA125; Liver metastasis; Pancreatic ductal adenocarcinoma; Prognosis; Unresectability.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflict of interest.
Figures
Similar articles
-
Preoperative CEA and CA 19-9 are prognostic markers for survival after curative resection for ductal adenocarcinoma of the pancreas - a retrospective tumor marker prognostic study.Int J Surg. 2013;11(10):1067-72. doi: 10.1016/j.ijsu.2013.10.005. Epub 2013 Oct 23. Int J Surg. 2013. PMID: 24161419
-
Synchronous resections of hepatic oligometastatic pancreatic cancer: Disputing a principle in a time of safe pancreatic operations in a retrospective multicenter analysis.Surgery. 2016 Jul;160(1):136-144. doi: 10.1016/j.surg.2016.02.019. Epub 2016 Apr 3. Surgery. 2016. PMID: 27048934
-
Radiofrequency ablation of liver metastasis in patients with locally controlled pancreatic ductal adenocarcinoma.J Vasc Interv Radiol. 2012 May;23(5):635-41. doi: 10.1016/j.jvir.2012.01.080. J Vasc Interv Radiol. 2012. PMID: 22525021
-
Synchronous surgery combined preoperative chemotherapy benefits patients suffering pancreatic ductal adenocarcinoma with liver metastases: a systematic review and meta-analysis.Sci Rep. 2025 Aug 4;15(1):28403. doi: 10.1038/s41598-025-13811-9. Sci Rep. 2025. PMID: 40759716 Free PMC article.
-
Different clinical presentations of metachronous pulmonary metastases after resection of pancreatic ductal adenocarcinoma: Retrospective study and review of the literature.World J Gastroenterol. 2017 Sep 21;23(35):6420-6428. doi: 10.3748/wjg.v23.i35.6420. World J Gastroenterol. 2017. PMID: 29085191 Free PMC article. Review.
Cited by
-
Pathological analysis of the superior mesenteric artery boundary in preoperative computed tomography of resectable pancreatic head adenocarcinoma.Oncol Lett. 2019 Jun;17(6):5711-5720. doi: 10.3892/ol.2019.10269. Epub 2019 Apr 18. Oncol Lett. 2019. PMID: 31186797 Free PMC article.
-
Surgical and local treatment of hepatic metastasis in pancreatic ductal adenocarcinoma: recent advances and future prospects.Ther Adv Med Oncol. 2020 Jun 23;12:1758835920933034. doi: 10.1177/1758835920933034. eCollection 2020. Ther Adv Med Oncol. 2020. PMID: 32636941 Free PMC article.
-
Defining oligometastatic pancreatic cancer: a systematic review and critical synthesis of consensus.ESMO Open. 2023 Dec;8(6):102067. doi: 10.1016/j.esmoop.2023.102067. Epub 2023 Nov 20. ESMO Open. 2023. PMID: 37988953 Free PMC article.
-
The risk factors for bone metastases in patients with colorectal cancer.Medicine (Baltimore). 2018 Oct;97(40):e12694. doi: 10.1097/MD.0000000000012694. Medicine (Baltimore). 2018. PMID: 30290664 Free PMC article.
-
Resection of isolated liver oligometastatic disease in pancreatic ductal adenocarcinoma: Is there a survival benefit? A systematic review.World J Gastrointest Surg. 2023 Jul 27;15(7):1512-1521. doi: 10.4240/wjgs.v15.i7.1512. World J Gastrointest Surg. 2023. PMID: 37555114 Free PMC article.
References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Michalski CW, Erkan M, Hüser N, Müller MW, Hartel M, Friess H, Kleeff J. Resection of primary pancreatic cancer and liver metastasis: a systematic review. Dig Surg. 2008;25:473–480. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
