

Clinical features of upper gastrointestinal serrated lesions: An endoscopy database analysis of 98746 patients
- PMID: 28018111
- PMCID: PMC5143750
- DOI: 10.3748/wjg.v22.i45.10038
Clinical features of upper gastrointestinal serrated lesions: An endoscopy database analysis of 98746 patients
Abstract
Aim: To analyse the clinical features of patients with the serrated lesions in the upper gastrointestinal tract (UPGI) tract.
Methods: Patients who underwent routine esophagogastroduodenoscopy (EGD) at the Digestive Endoscopy Centre of General Hospital, Tianjin Medical University between January 2011 and December 2015 were consecutively recruited. Patients with UPGI serrated lesions were consecutively identified. The patients' demographics and histopathology were recorded. The colorectal findings for patients who underwent colonoscopy simultaneously or within six months were also extracted from the colonoscopy database. In addition, we analysed differences in colorectal neoplasia detection between the study patients and randomly selected patients matched for age and gender who did not exhibit serrated lesions and who also underwent colonoscopy in the same period.
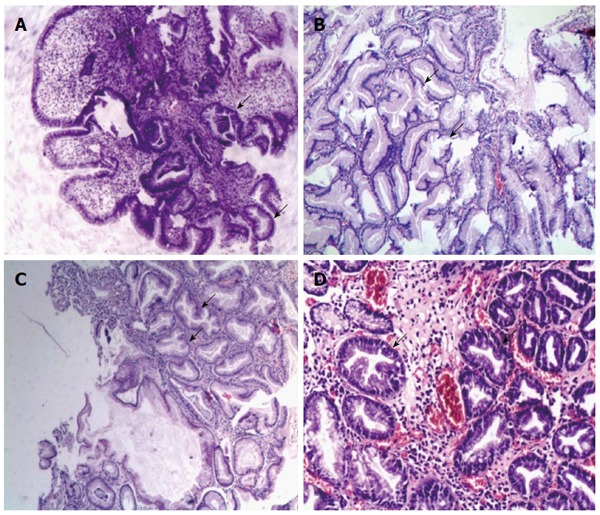
Results: A total of 21 patients out of 98746 patients (0.02%) who underwent EGD were confirmed to have serrated lesions with predominantly crenated, sawtooth-like configurations. The mean age of the 21 patients was (55.3 ± 17.2) years, and 11 patients were male (52.4%). In terms of the locations of the serrated lesions, 17 were found in the stomach (including 3 in the cardia, 9 in the corpus and 5 in the antrum), 3 were found in the duodenum, and 1 was found in the esophagus. Serrated lesions were found in different mucosal lesions, with 14 lesions were detected in polyps (8 hyperplastic polyps and 6 serrated adenomas with low grade dysplasia), 3 detected in Ménétrier gastropathy, 3 detected in an area of inflammation or ulcer, and 1 detected in the intramucosal carcinoma of the duodenum. In addition, colonoscopy data were available for 18 patients, and a significantly higher colorectal adenoma detection rate was observed in the UPGI serrated lesions group than in the randomly selected age- and gender-matched group without serrated lesions who also underwent colonoscopy in the same period (38.9% vs 11.1%, OR = 5.091, 95%CI: 1.534-16.890, P = 0.010). The detection rate of advanced adenoma was also higher in the UPGI serrated lesions group (22.2% vs 4.2%, OR = 6.571, 95%CI: 1.322-32.660, P = 0.028).
Conclusion: Serrated lesions in the UPGI were detected in various mucosal lesions with different pathological morphologies. Moreover colonoscopy is recommended for the detection of concurrent colorectal adenoma for these patients.
Keywords: Clinical features; Colorectal adenoma; Colorectal cancer; Serrated lesions; Upper gastrointestinal tract.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest.
Figures
Similar articles
-
Findings in the distal colorectum are not associated with proximal advanced serrated lesions.Clin Gastroenterol Hepatol. 2015 Feb;13(2):345-51. doi: 10.1016/j.cgh.2014.07.044. Epub 2014 Jul 30. Clin Gastroenterol Hepatol. 2015. PMID: 25083562
-
[Distribution characteristics and risk factors of colorectal adenomas].Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Jun 25;21(6):678-684. Zhonghua Wei Chang Wai Ke Za Zhi. 2018. PMID: 29968244 Chinese.
-
Prevalence of serrated polyps and association with synchronous advanced neoplasia in screening colonoscopy.Endoscopy. 2014 Mar;46(3):219-24. doi: 10.1055/s-0033-1358800. Epub 2013 Nov 19. Endoscopy. 2014. PMID: 24254386
-
Traditional serrated adenomas of the upper digestive tract.J Clin Pathol. 2016 Jan;69(1):1-5. doi: 10.1136/jclinpath-2015-203258. Epub 2015 Oct 14. J Clin Pathol. 2016. PMID: 26468393 Free PMC article. Review.
-
Serrated polyps: critical precursors to colorectal cancer.Expert Rev Gastroenterol Hepatol. 2011 Oct;5(5):627-35. doi: 10.1586/egh.11.67. Expert Rev Gastroenterol Hepatol. 2011. PMID: 21910580 Review.
Cited by
-
Two duodenal sessile serrated lesions in a patient with serrated polyposis syndrome: case report and review of the literature.Clin J Gastroenterol. 2025 Jul 11. doi: 10.1007/s12328-025-02165-4. Online ahead of print. Clin J Gastroenterol. 2025. PMID: 40643790
-
Blue laser magnifying endoscopy in the diagnosis of chronic gastritis.Exp Ther Med. 2019 Sep;18(3):1993-2000. doi: 10.3892/etm.2019.7811. Epub 2019 Jul 25. Exp Ther Med. 2019. PMID: 31452698 Free PMC article.
-
Gastric and small intestinal traditional serrated adenomas: a detailed morphologic and immunohistochemical analysis.Turk J Gastroenterol. 2020 Jun;31(6):441-450. doi: 10.5152/tjg.2020.19931. Turk J Gastroenterol. 2020. PMID: 32721915 Free PMC article.
-
Spatially resolved multi-omics highlights cell-specific metabolic remodeling and interactions in gastric cancer.Nat Commun. 2023 May 10;14(1):2692. doi: 10.1038/s41467-023-38360-5. Nat Commun. 2023. PMID: 37164975 Free PMC article.
References
-
- Jass JR, Smith M. Sialic acid and epithelial differentiation in colorectal polyps and cancer--a morphological, mucin and lectin histochemical study. Pathology. 1992;24:233–242. - PubMed
-
- Bordaçahar B, Barret M, Terris B, Dhooge M, Dreanic J, Prat F, Coriat R, Chaussade S. Sessile serrated adenoma: from identification to resection. Dig Liver Dis. 2015;47:95–102. - PubMed
-
- Burgess NG, Tutticci NJ, Pellise M, Bourke MJ. Sessile serrated adenomas/polyps with cytologic dysplasia: a triple threat for interval cancer. Gastrointest Endosc. 2014;80:307–310. - PubMed
-
- Huang CS, Farraye FA, Yang S, O’Brien MJ. The clinical significance of serrated polyps. Am J Gastroenterol. 2011;106:229–240; quiz 241. - PubMed
-
- O’Brien MJ, Zhao Q, Yang S. Colorectal serrated pathway cancers and precursors. Histopathology. 2015;66:49–65. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
