

Distinctive Steady-State Heart Rate and Blood Pressure Responses to Passive Robotic Leg Exercise and Functional Electrical Stimulation during Head-Up Tilt
- PMID: 28018240
- PMCID: PMC5145897
- DOI: 10.3389/fphys.2016.00612
Distinctive Steady-State Heart Rate and Blood Pressure Responses to Passive Robotic Leg Exercise and Functional Electrical Stimulation during Head-Up Tilt
Abstract
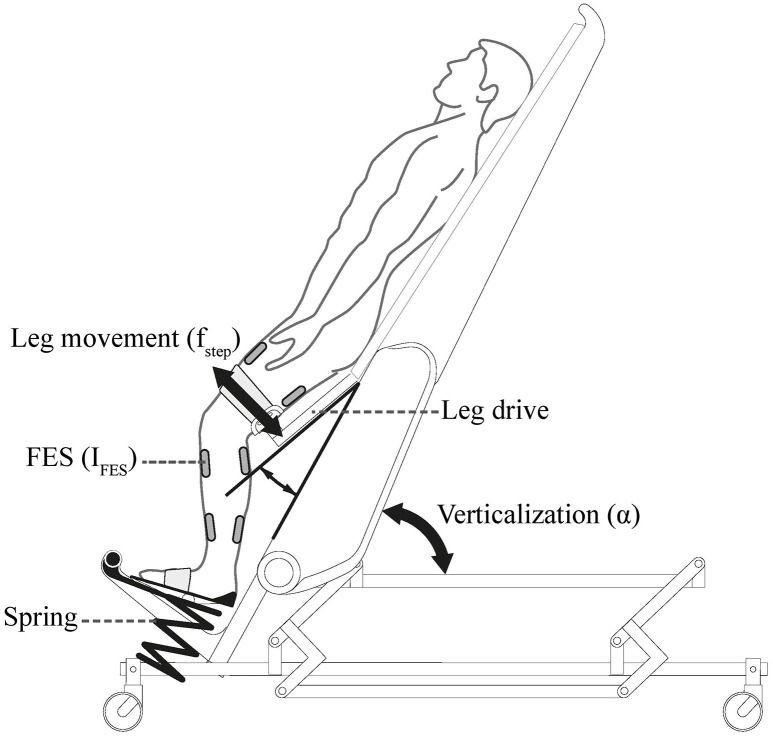
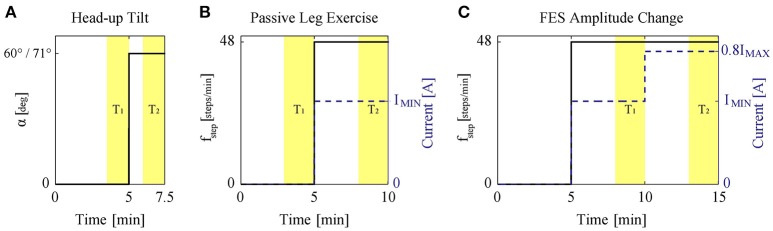
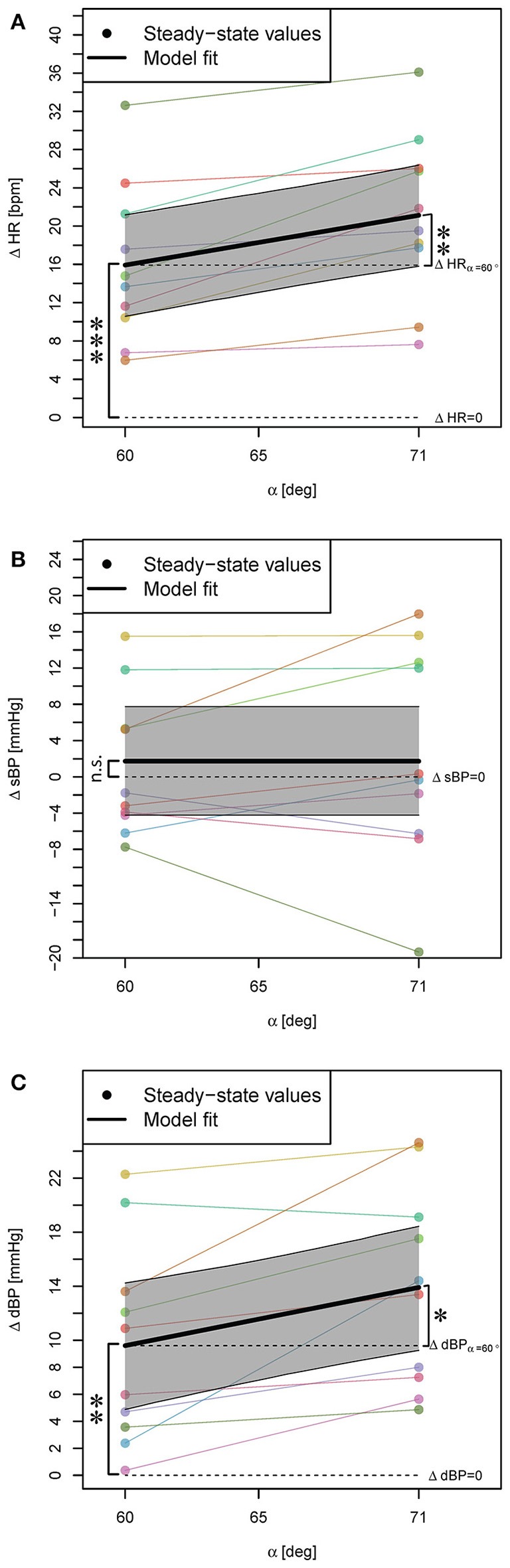
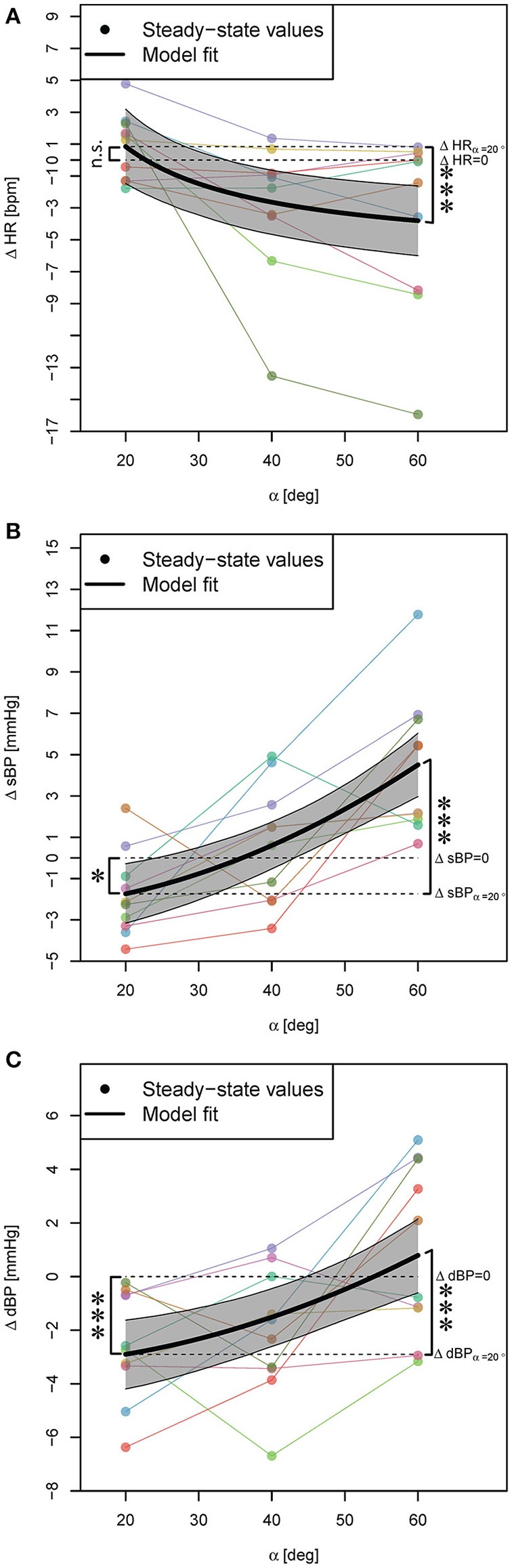
Introduction: Tilt tables enable early mobilization of patients by providing verticalization. But there is a high risk of orthostatic hypotension provoked by verticalization, especially after neurological diseases such as spinal cord injury. Robot-assisted tilt tables might be an alternative as they add passive robotic leg exercise (PE) that can be enhanced with functional electrical stimulation (FES) to the verticalization, thus reducing the risk of orthostatic hypotension. We hypothesized that the influence of PE on the cardiovascular system during verticalization (i.e., head-up tilt) depends on the verticalization angle, and FES strengthens the PE influence. To test our hypotheses, we investigated the PE effects on the cardiovascular parameters heart rate (HR), and systolic and diastolic blood pressures (sBP, dBP) at different angles of verticalization in a healthy population. Methods: Ten healthy subjects on a robot-assisted tilt table underwent four different study protocols while HR, sBP, and dBP were measured: (1) head-up tilt to 60° and 71° without PE; (2) PE at 20°, 40°, and 60° of head-up tilt; (3) PE while constant FES intensity was applied to the leg muscles, at 20°, 40°, and 60° of head-up tilt; (4) PE with variation of the applied FES intensity at 0°, 20°, 40°, and 60° of head-up tilt. Linear mixed models were used to model changes in HR, sBP, and dBP responses. Results: The models show that: (1) head-up tilt alone resulted in statistically significant increases in HR and dBP, but no change in sBP. (2) PE during head-up tilt resulted in statistically significant changes in HR, sBP, and dBP, but not at each angle and not always in the same direction (i.e., increase or decrease of cardiovascular parameters). Neither adding (3) FES at constant intensity to PE nor (4) variation of FES intensity during PE had any statistically significant effects on the cardiovascular parameters. Conclusion: The effect of PE on the cardiovascular system during head-up tilt is strongly dependent on the verticalization angle. Therefore, we conclude that orthostatic hypotension cannot be prevented by PE alone, but that the preventive effect depends on the verticalization angle of the robot-assisted tilt table. FES (independent of intensity) is not an important contributing factor to the PE effect.
Keywords: cardiovascular system; functional electrical stimulation (FES); linear mixed models; orthostatic hypotension; parametric bootstrap; rehabilitation robotics; robotic tilt table.
Figures
Similar articles
-
Distinctive Steady-State Heart Rate and Blood Pressure Responses to Passive Robotic Leg Exercise during Head-Up Tilt: A Pilot Study in Neurological Patients.Front Physiol. 2017 Jun 2;8:327. doi: 10.3389/fphys.2017.00327. eCollection 2017. Front Physiol. 2017. PMID: 28626427 Free PMC article.
-
The effects of lower-extremity functional electric stimulation on the orthostatic responses of people with tetraplegia.Arch Phys Med Rehabil. 2005 Jul;86(7):1427-33. doi: 10.1016/j.apmr.2004.12.033. Arch Phys Med Rehabil. 2005. PMID: 16003676
-
Cardiovascular response to functional electrical stimulation and dynamic tilt table therapy to improve orthostatic tolerance.J Electromyogr Kinesiol. 2008 Dec;18(6):900-7. doi: 10.1016/j.jelekin.2008.08.007. Epub 2008 Oct 2. J Electromyogr Kinesiol. 2008. PMID: 18835189
-
Hemodynamic Response to the Head-Up Tilt Test in Patients With Syncope as a Predictor of the Test Outcome: A Meta-Analysis Approach.Front Physiol. 2019 Mar 7;10:184. doi: 10.3389/fphys.2019.00184. eCollection 2019. Front Physiol. 2019. PMID: 30899228 Free PMC article.
-
[Verticalization as a factor of early rehabilitation in the patients with a spinal cord injury].Vopr Kurortol Fizioter Lech Fiz Kult. 2013 Jul-Aug;(4):47-52. Vopr Kurortol Fizioter Lech Fiz Kult. 2013. PMID: 24137937 Review. Russian.
Cited by
-
Distinctive Steady-State Heart Rate and Blood Pressure Responses to Passive Robotic Leg Exercise during Head-Up Tilt: A Pilot Study in Neurological Patients.Front Physiol. 2017 Jun 2;8:327. doi: 10.3389/fphys.2017.00327. eCollection 2017. Front Physiol. 2017. PMID: 28626427 Free PMC article.
-
Modeling the effect of tilting, passive leg exercise, and functional electrical stimulation on the human cardiovascular system.Med Biol Eng Comput. 2017 Sep;55(9):1693-1708. doi: 10.1007/s11517-017-1628-8. Epub 2017 Feb 10. Med Biol Eng Comput. 2017. PMID: 28188470
-
Intervention Effect of Rehabilitation Robotic Bed Under Machine Learning Combined With Intensive Motor Training on Stroke Patients With Hemiplegia.Front Neurorobot. 2022 Jun 9;16:865403. doi: 10.3389/fnbot.2022.865403. eCollection 2022. Front Neurorobot. 2022. PMID: 35756160 Free PMC article.
-
Cardiovascular responses to leg muscle loading during head-down tilt at rest and after dynamic exercises.Sci Rep. 2019 Feb 26;9(1):2804. doi: 10.1038/s41598-019-39360-6. Sci Rep. 2019. PMID: 30808948 Free PMC article.
-
Cardiovascular responses to leg-press exercises during head-down tilt.Front Sports Act Living. 2024 Aug 27;6:1396391. doi: 10.3389/fspor.2024.1396391. eCollection 2024. Front Sports Act Living. 2024. PMID: 39290333 Free PMC article.
References
-
- Adami A., Pizzinelli P., Bringard A., Capelli C., Malacarne M., Lucini D., et al. . (2013). Cardiovascular re-adjustments and baroreflex response during clinical reambulation procedure at the end of 35-day bed rest in humans. Appl. Physiol. Nutr. Metab. 38, 673–680. 10.1139/apnm-2012-0396 - DOI - PubMed
-
- Bates D., Mächler M., Bolker B., Walker S. (2014). Fitting linear mixed-effects models using lme4. arXiv:1406.5823. - PubMed
-
- Bourdin G., Barbier J., Burlem J.-F., Durante G., Passant S., Vincent B., et al. . (2010). The feasibility of early physical activity in intensive care unit patients: a prospective observational one-center study. Respir. Care 55, 400–407. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous