

Intra-Attack Vestibuloocular Reflex Changes in Ménière's Disease
- PMID: 28018691
- PMCID: PMC5149633
- DOI: 10.1155/2016/2427983
Intra-Attack Vestibuloocular Reflex Changes in Ménière's Disease
Abstract
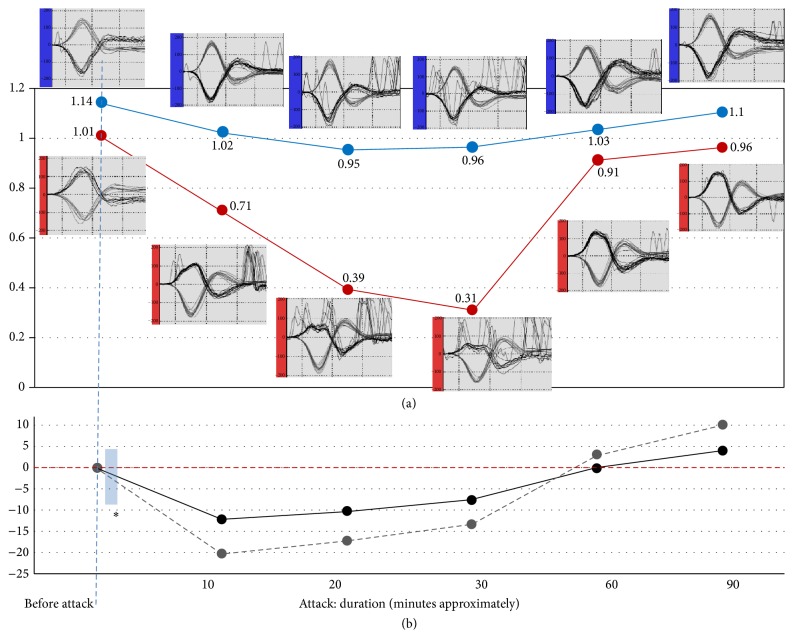
Ménière's attack has been shown to temporarily alter the vestibuloocular reflex (VOR). A patient with unilateral Ménière's disease was serially evaluated with the video Head Impulse Test during single, untreated episodes of acute vertigo. Spontaneous nystagmus activity was concurrently recorded in order to establish the three typical phases of Ménière's attack (irritative, paralytic, and recovery) and correlate them with VOR performance. The onset of attack was associated with a quick change in VOR gain on the side of the affected ear. While a rapidly progressive reduction of the VOR was evident at the paralytic nystagmus phase, in the recovery phase the VOR gain returned to normal and the direction of the previous nystagmus reversed. The membrane rupture potassium intoxication theory provides a good foundation with which to explain these dynamic VOR changes and the observed triphasic direction behavior of the spontaneous nystagmus. We additionally postulated that endolymphatic fluid displacement could have a synergic effect during the earliest phase of attack.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
Similar articles
-
Fluctuating Vestibulo-Ocular Reflex in Ménière's Disease.Otol Neurotol. 2017 Feb;38(2):244-247. doi: 10.1097/MAO.0000000000001298. Otol Neurotol. 2017. PMID: 27926585
-
A Puzzle of Vestibular Physiology in a Meniere's Disease Acute Attack.Case Rep Otolaryngol. 2015;2015:460757. doi: 10.1155/2015/460757. Epub 2015 Jun 18. Case Rep Otolaryngol. 2015. PMID: 26167320 Free PMC article.
-
Rat Model of Ménière's Attack: Intratympanic Injection of Potassium Chloride Produces Direction-Changing Spontaneous Nystagmus and Hearing Fluctuations.Audiol Neurootol. 2019;24(5):217-223. doi: 10.1159/000502275. Epub 2019 Sep 13. Audiol Neurootol. 2019. PMID: 31522181
-
Saccular otoconia as a cause of Ménière's disease: hypothesis based on two theories.J Laryngol Otol. 2018 Sep;132(9):771-774. doi: 10.1017/S0022215118001366. Epub 2018 Aug 28. J Laryngol Otol. 2018. PMID: 30149814 Review.
-
Acute unilateral loss of vestibular function.Handb Clin Neurol. 2016;137:219-29. doi: 10.1016/B978-0-444-63437-5.00015-7. Handb Clin Neurol. 2016. PMID: 27638073 Review.
Cited by
-
Neurological update: neuro-otology 2023.J Neurol. 2023 Dec;270(12):6170-6192. doi: 10.1007/s00415-023-11922-9. Epub 2023 Aug 17. J Neurol. 2023. PMID: 37592138 Free PMC article.
-
Evolution of Vestibular Findings During and Between the Attacks of Meniere Disease: Update.Neurol Clin Pract. 2024 Apr;14(2):e200235. doi: 10.1212/CPJ.0000000000200235. Epub 2024 Jan 10. Neurol Clin Pract. 2024. PMID: 38223349 Free PMC article. Review.
-
Enhanced Eye Velocity in Head Impulse Testing-A Possible Indicator of Endolymphatic Hydrops.Front Surg. 2021 May 7;8:666390. doi: 10.3389/fsurg.2021.666390. eCollection 2021. Front Surg. 2021. PMID: 34026816 Free PMC article.
-
Usefulness of Video Head Impulse Test Results in the Identification of Meniere's Disease.Front Neurol. 2020 Oct 29;11:581527. doi: 10.3389/fneur.2020.581527. eCollection 2020. Front Neurol. 2020. PMID: 33193038 Free PMC article. Review.
-
The Role of Mobile Phone Camera Recordings in the Diagnosis of Meniere's Disease and Pathophysiological Implications.J Int Adv Otol. 2020 Apr;16(1):18-23. doi: 10.5152/iao.2019.6605. J Int Adv Otol. 2020. PMID: 32066548 Free PMC article. Clinical Trial.
References
-
- Bance M., Mai M., Tomlinson D., Rutka J. The changing direction of nystagmus in acute Meniere's disease: pathophysiological implications. Laryngoscope. 1991;101(2):197–201. - PubMed
-
- Aw S. T., Haslwanter T., Halmagyi G. M., Curthoys I. S., Yavor R. A., Todd M. J. Three-dimensional vector analysis of the human vestibuloocular reflex in response to high-acceleration head rotations: I. Responses in normal subjects. Journal of Neurophysiology. 1996;76(6):4009–4020. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
