

Tissue-Associated Bacterial Alterations in Rectal Carcinoma Patients Revealed by 16S rRNA Community Profiling
- PMID: 28018861
- PMCID: PMC5145865
- DOI: 10.3389/fcimb.2016.00179
Tissue-Associated Bacterial Alterations in Rectal Carcinoma Patients Revealed by 16S rRNA Community Profiling
Abstract
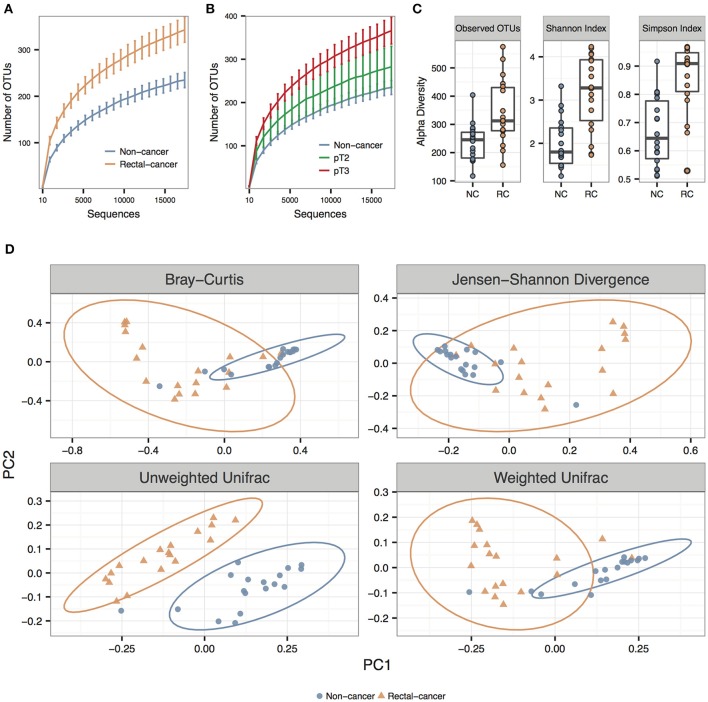
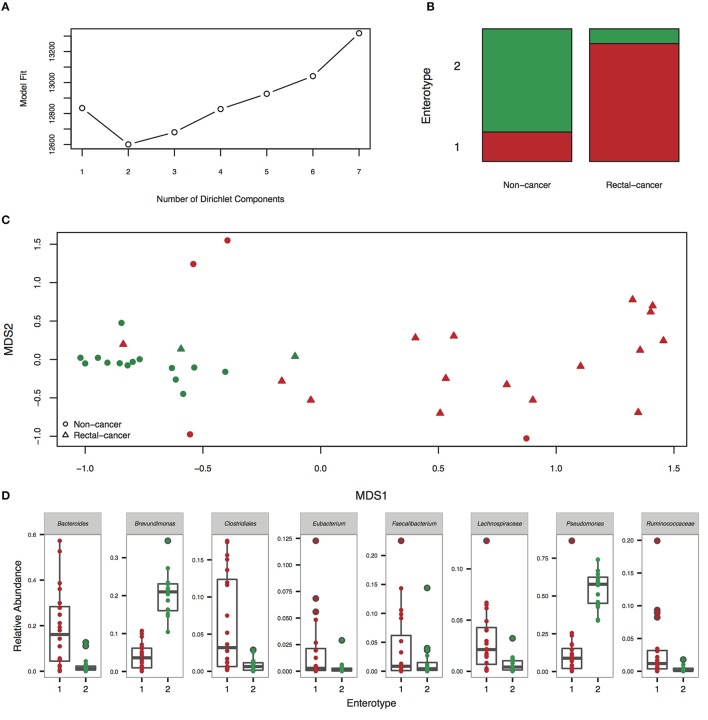
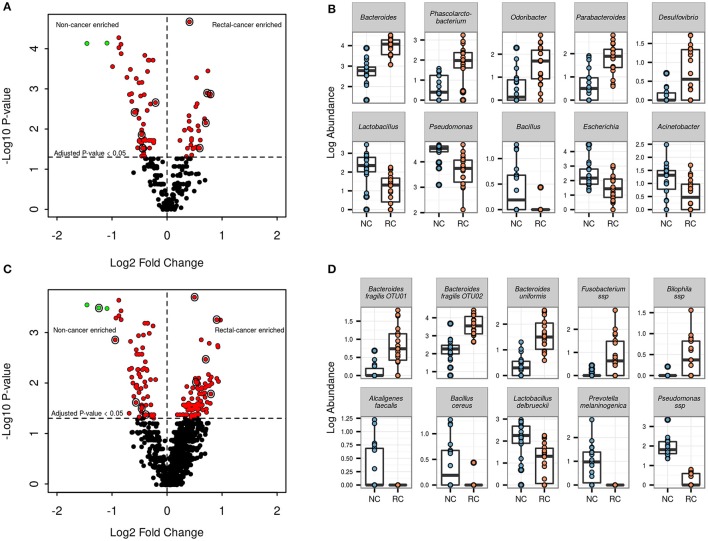
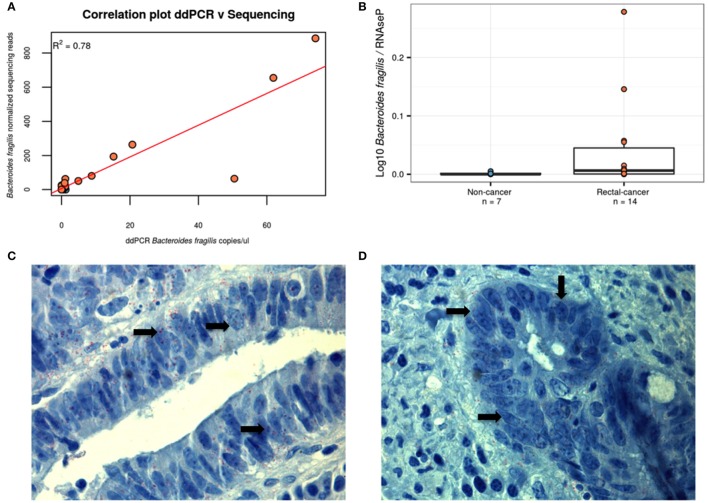
Sporadic and inflammatory forms of colorectal cancer (CRC) account for more than 80% of cases. Recent publications have shown mechanistic evidence for the involvement of gut bacteria in the development of both CRC-forms. Whereas, colon and rectal cancer have been routinely studied together as CRC, increasing evidence show these to be distinct diseases. Also, the common use of fecal samples to study microbial communities may reflect disease state but possibly not the tumor microenvironment. We performed this study to evaluate differences in bacterial communities found in tissue samples of 18 rectal-cancer subjects when compared to 18 non-cancer controls. Samples were collected during exploratory colonoscopy (non-cancer group) or during surgery for tumor excision (rectal-cancer group). High throughput 16S rRNA amplicon sequencing of the V4-V5 region was conducted on the Ion PGM platform, reads were filtered using Qiime and clustered using UPARSE. We observed significant increases in species richness and diversity in rectal cancer samples, evidenced by the total number of OTUs and the Shannon and Simpson indexes. Enterotyping analysis divided our cohort into two groups, with the majority of rectal cancer samples clustering into one enterotype, characterized by a greater abundance of Bacteroides and Dorea. At the phylum level, rectal-cancer samples had increased abundance of candidate phylum OD1 (also known as Parcubacteria) whilst non-cancer samples had increased abundance of Planctomycetes. At the genera level, rectal-cancer samples had higher abundances of Bacteroides, Phascolarctobacterium, Parabacteroides, Desulfovibrio, and Odoribacter whereas non-cancer samples had higher abundances of Pseudomonas, Escherichia, Acinetobacter, Lactobacillus, and Bacillus. Two Bacteroides fragilis OTUs were more abundant among rectal-cancer patients seen through 16S rRNA amplicon sequencing, whose presence was confirmed by immunohistochemistry and enrichment verified by digital droplet PCR. Our findings point to increased bacterial richness and diversity in rectal cancer, along with several differences in microbial community composition. Our work is the first to present evidence for a possible role of bacteria such as B. fragilis and the phylum Parcubacteria in rectal cancer, emphasizing the need to study tissue-associated bacteria and specific regions of the gastrointestinal tract in order to better understand the possible links between the microbiota and rectal cancer.
Keywords: 16S rRNA gene sequencing; Bacterial diversity and community composition; Bacteroides fragilis; mucosa-associated microbiota; rectal cancer.
Figures
Similar articles
-
Diversity of Duodenal and Rectal Microbiota in Biopsy Tissues and Luminal Contents in Healthy Volunteers.J Microbiol Biotechnol. 2015 Jul;25(7):1136-45. doi: 10.4014/jmb.1412.12047. J Microbiol Biotechnol. 2015. PMID: 25737115
-
Capturing the diversity of the human gut microbiota through culture-enriched molecular profiling.Genome Med. 2016 Jul 1;8(1):72. doi: 10.1186/s13073-016-0327-7. Genome Med. 2016. PMID: 27363992 Free PMC article.
-
High-throughput sequencing of 16S rRNA Gene Reveals Substantial Bacterial Diversity on the Municipal Dumpsite.BMC Microbiol. 2016 Jul 11;16(1):145. doi: 10.1186/s12866-016-0758-8. BMC Microbiol. 2016. PMID: 27400733 Free PMC article.
-
Deciphering Diversity Indices for a Better Understanding of Microbial Communities.J Microbiol Biotechnol. 2017 Dec 28;27(12):2089-2093. doi: 10.4014/jmb.1709.09027. J Microbiol Biotechnol. 2017. PMID: 29032640 Review.
-
Gut Microbiota Profile in Patients with Type 1 Diabetes Based on 16S rRNA Gene Sequencing: A Systematic Review.Dis Markers. 2020 Aug 27;2020:3936247. doi: 10.1155/2020/3936247. eCollection 2020. Dis Markers. 2020. PMID: 32908614 Free PMC article.
Cited by
-
Gut microbiome identifies risk for colorectal polyps.BMJ Open Gastroenterol. 2019 May 27;6(1):e000297. doi: 10.1136/bmjgast-2019-000297. eCollection 2019. BMJ Open Gastroenterol. 2019. PMID: 31275588 Free PMC article.
-
The Role of Gut Microbiome Perturbation in Fatigue Induced by Repeated Stress from Chemoradiotherapy: A Proof of Concept Study.Adv Med. 2020 Feb 7;2020:6375876. doi: 10.1155/2020/6375876. eCollection 2020. Adv Med. 2020. PMID: 32090133 Free PMC article.
-
Effect of Marine-Derived Scallop Peptide Hydrolysate on Immune Modulation and Gut Microbiota Restoration in Cyclophosphamide-Induced Immunosuppressed Mice.Food Sci Nutr. 2025 Jul 23;13(7):e70421. doi: 10.1002/fsn3.70421. eCollection 2025 Jul. Food Sci Nutr. 2025. PMID: 40703615 Free PMC article.
-
Alterations in the Gut Microbiota and Their Metabolites in Colorectal Cancer: Recent Progress and Future Prospects.Front Oncol. 2022 Feb 11;12:841552. doi: 10.3389/fonc.2022.841552. eCollection 2022. Front Oncol. 2022. PMID: 35223525 Free PMC article. Review.
-
The effect of exposure to high altitude and low oxygen on intestinal microbial communities in mice.PLoS One. 2018 Sep 12;13(9):e0203701. doi: 10.1371/journal.pone.0203701. eCollection 2018. PLoS One. 2018. PMID: 30208088 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical