

3D Volumetric Modeling and Microvascular Reconstruction of Irradiated Lumbosacral Defects after Oncologic Resection
- PMID: 28018904
- PMCID: PMC5153530
- DOI: 10.3389/fsurg.2016.00066
3D Volumetric Modeling and Microvascular Reconstruction of Irradiated Lumbosacral Defects after Oncologic Resection
Abstract
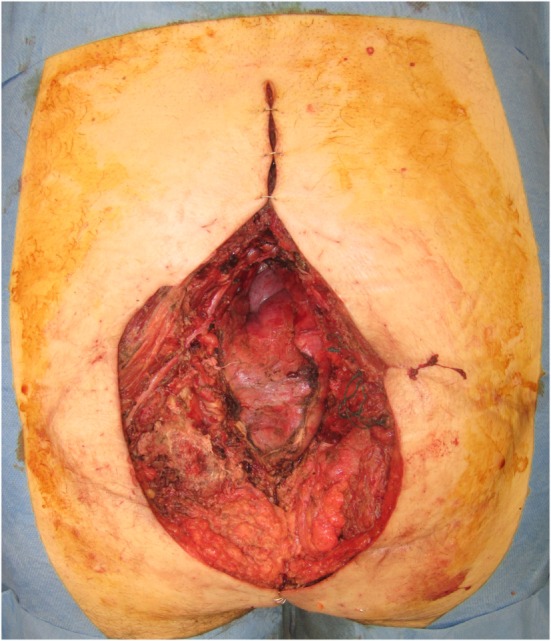
Background: Locoregional flaps are sufficient in most sacral reconstructions. However, large sacral defects due to malignancy necessitate a different reconstructive approach, with local flaps compromised by radiation and regional flaps inadequate for broad surface areas or substantial volume obliteration. In this report, we present our experience using free muscle transfer for volumetric reconstruction, in such cases, and demonstrate three-dimensional (3D) haptic models of the sacral defect to aid preoperative planning.
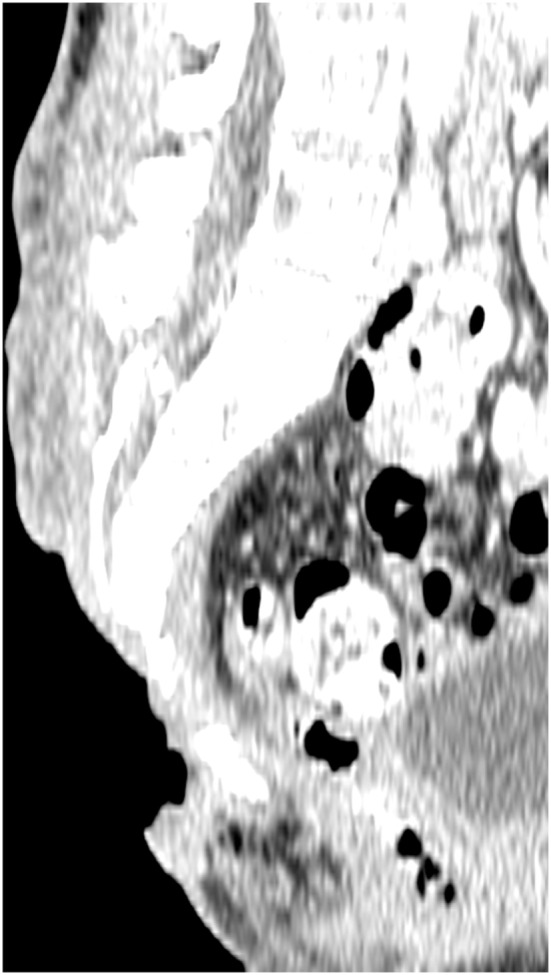
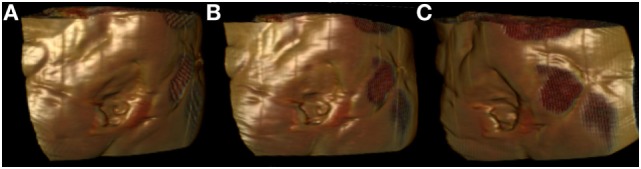
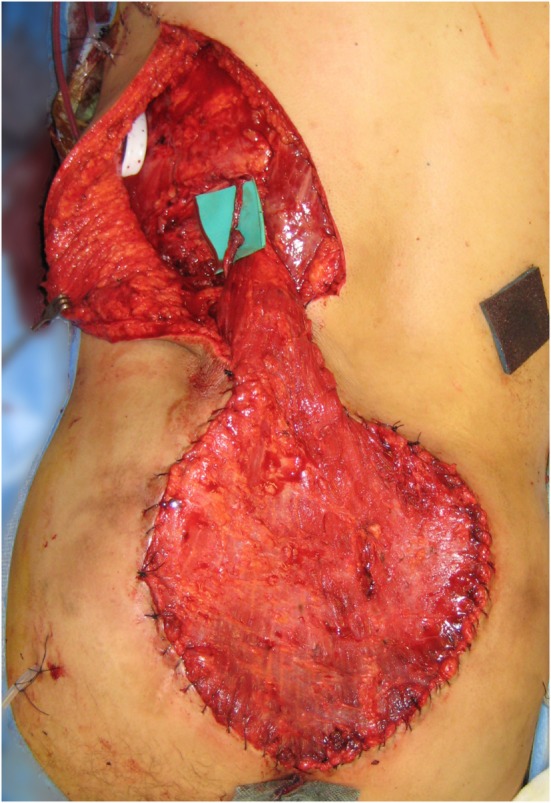
Methods: Five consecutive patients with irradiated sacral defects secondary to oncologic resections were included, surface area ranging from 143-600 cm2. Latissimus dorsi (LD)-based free flap sacral reconstruction was performed in each case, between 2005 and 2011. Where the superior gluteal artery was compromised, the subcostal artery (SA) was used as a recipient vessel. Microvascular technique, complications, and outcomes are reported. The use of volumetric analysis and 3D printing is also demonstrated, with imaging data converted to 3D images suitable for 3D printing with Osirix software (Pixmeo, Geneva, Switzerland). An office-based, desktop 3D printer was used to print 3D models of sacral defects, used to demonstrate surface area and contour and produce a volumetric print of the dead space needed for flap obliteration.
Results: The clinical series of LD free flap reconstructions is presented, with successful transfer in all cases, and adequate soft-tissue cover and volume obliteration achieved. The original use of the SA as a recipient vessel was successfully achieved. All wounds healed uneventfully. 3D printing is also demonstrated as a useful tool for 3D evaluation of volume and dead space.
Conclusion: Free flaps offer unique benefits in sacral reconstruction where local tissue is compromised by irradiation and tumor recurrence, and dead space requires accurate volumetric reconstruction. We describe for the first time the use of the SA as a recipient in free flap sacral reconstruction. 3D printing of haptic bio-models is a rapidly evolving field with a substantial role in preoperative planning.
Keywords: free flap; model; planning; preoperative imaging; volumetric analysis.
Figures





Similar articles
-
A Standard Algorithm for Reconstruction of Scalp Defects With Simultaneous Free Flaps in an Interdisciplinary Two-Team Approach.Front Oncol. 2019 Oct 25;9:1130. doi: 10.3389/fonc.2019.01130. eCollection 2019. Front Oncol. 2019. PMID: 31709189 Free PMC article.
-
3D volumetric analysis for planning breast reconstructive surgery.Breast Cancer Res Treat. 2014 Jul;146(2):457-60. doi: 10.1007/s10549-014-3028-1. Epub 2014 Jun 18. Breast Cancer Res Treat. 2014. PMID: 24939062
-
Muscle-splitting approach to superior and inferior gluteal vessels: versatile source of recipient vessels for free-tissue transfer to sacral, gluteal, and ischial regions.Plast Reconstr Surg. 2000 Jul;106(1):81-6. doi: 10.1097/00006534-200007000-00015. Plast Reconstr Surg. 2000. PMID: 10883616
-
OsiriX software as a preoperative planning tool in cranial neurosurgery: A step-by-step guide for neurosurgical residents.Surg Neurol Int. 2017 Oct 10;8:241. doi: 10.4103/sni.sni_419_16. eCollection 2017. Surg Neurol Int. 2017. PMID: 29119039 Free PMC article. Review.
-
3D haptic modelling for preoperative planning of hepatic resection: A systematic review.Ann Med Surg (Lond). 2016 Jul 12;10:1-7. doi: 10.1016/j.amsu.2016.07.002. eCollection 2016 Sep. Ann Med Surg (Lond). 2016. PMID: 27489617 Free PMC article. Review.
Cited by
-
The utility of three-dimensional models in complex microsurgical reconstruction.Arch Plast Surg. 2020 Sep;47(5):428-434. doi: 10.5999/aps.2020.00829. Epub 2020 Sep 15. Arch Plast Surg. 2020. PMID: 32971594 Free PMC article.
-
Emerging Applications of Bedside 3D Printing in Plastic Surgery.Front Surg. 2015 Jun 16;2:25. doi: 10.3389/fsurg.2015.00025. eCollection 2015. Front Surg. 2015. PMID: 26137465 Free PMC article. Review.
-
Exploring Age-Related Variations in Carpal Bone Volume: Implications for Clinical Practice and Anatomical Understanding.Hand (N Y). 2025 Sep;20(6):951-957. doi: 10.1177/15589447241242830. Epub 2024 Apr 12. Hand (N Y). 2025. PMID: 38606949 Free PMC article.
-
Challenging the Dogma of Dead Space Obliteration With Muscle Flaps in Deep Spinal Surgical Site Infections.Plast Reconstr Surg Glob Open. 2025 May 1;13(5):e6732. doi: 10.1097/GOX.0000000000006732. eCollection 2025 May. Plast Reconstr Surg Glob Open. 2025. PMID: 40321322 Free PMC article.
References
-
- Chae MP, Hunter-Smith DJ, Rozen WM. Image-guided 3D-printing and haptic modeling in plastic surgery. In: Saba L, Rozen WM, Alonso-Burgos A, Ribuffo D, editors. Imaging in Plastic Surgery. London, UK: CRC Taylor and Francis Press; (2014). p. 819–30.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials