

Spinal Epidural Abscess in Adults: A 10-Year Clinical Experience at a Tertiary Care Academic Medical Center
- PMID: 28018923
- PMCID: PMC5172511
- DOI: 10.1093/ofid/ofw191
Spinal Epidural Abscess in Adults: A 10-Year Clinical Experience at a Tertiary Care Academic Medical Center
Abstract
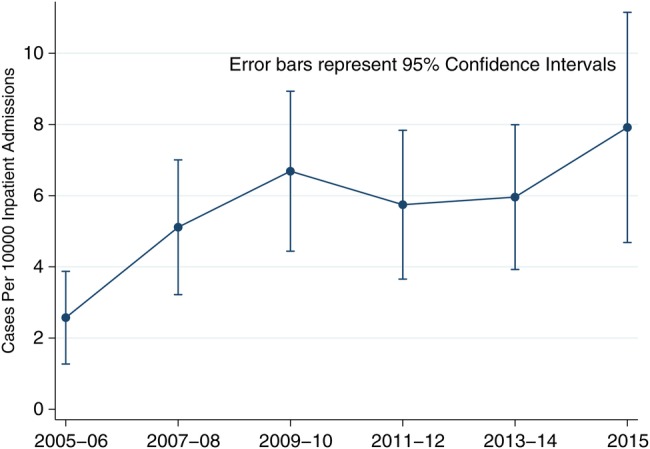
Background. Delayed recognition of spinal epidural abscess (SEA) contributes to poor outcomes from this highly morbid and potentially lethal infection. We performed a case-control study in a regional, high-volume, tertiary care, academic medical center over the years 2005-2015 to assess the potential changing epidemiology, clinical and laboratory manifestations, and course of this disorder and to identify factors that might lead to early identification of SEA. Methods. Diagnostic billing codes consistent with SEA were used to identify inpatient admissions for abstraction. Subjects were categorized as cases or controls based on the results of spinal imaging studies. Characteristics were compared using Fisher's exact or Kruskal-Wallis tests. All P values were 2-sided with a critical threshold of <.05. Results. We identified 162 cases and 88 controls during the study period. The incidence of SEA increased from 2.5 to 8.0 per 10 000 admissions, a 3.3-fold change from 2005 to 2015 (P < .001 for the linear trend). Compared with controls, cases were significantly more likely to have experienced at least 1 previous healthcare visit or received antimicrobials within 30 days of admission; to have comorbidities of injection drug use, alcohol abuse, or obesity; and to manifest fever or rigors. Cases were also more likely to harbor coinfection at a noncontiguous site. When available, inflammatory markers were noted to be markedly elevated in cases. Focal neurologic deficits were seen with similar frequencies in both groups. Conclusions. Based on our analysis, it appears that selected factors noted at the time of clinical presentation may facilitate early recognition of SEA.
Keywords: CNS infection; spinal epidural abscess.
© The Author 2016. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures
References
-
- Darouiche RO. Spinal epidural abscess. N Engl J Med 2006; 355:2012–20. - PubMed
-
- Davis DP, Wold RM, Patel RJ et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med 2004; 26:285–91. - PubMed
-
- Nussbaum ES, Rigamonti D, Standiford H et al. Spinal epidural abscess: a report of 40 cases and review. Surg Neurol 1992; 38:225–31. - PubMed
-
- Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev 2000; 23:175–204. - PubMed
-
- Shweikeh F, Saeed K, Bukavina L et al. An institutional series and contemporary review of bacterial spinal epidural abscess: current status and future directions. Neurosurg Focus 2014; 37:E9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
