

EGFR Gene Amplification and KRAS Mutation Predict Response to Combination Targeted Therapy in Metastatic Colorectal Cancer
- PMID: 28025786
- PMCID: PMC5451302
- DOI: 10.1007/s12253-016-0166-2
EGFR Gene Amplification and KRAS Mutation Predict Response to Combination Targeted Therapy in Metastatic Colorectal Cancer
Abstract
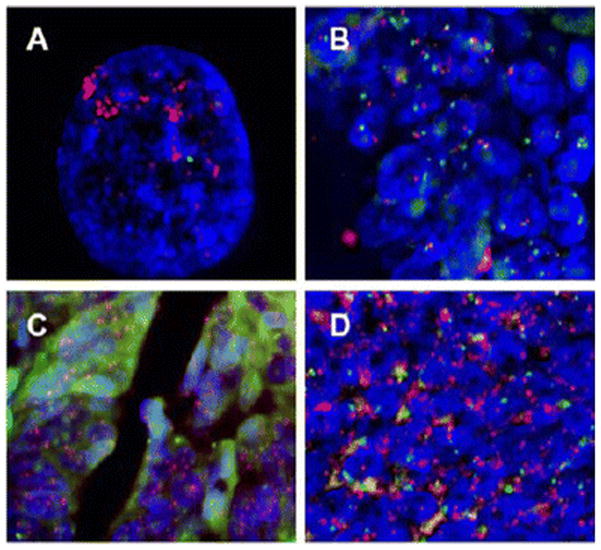
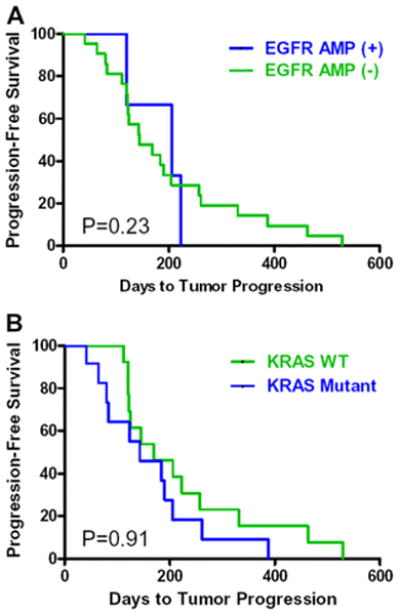
Genetic variability in KRAS and EGFR predicts response to cetuximab in irinotecan refractory colorectal cancer. Whether these markers or others remain predictive in combination biologic therapies including bevacizumab is unknown. We identified predictive biomarkers from patients with irinotecan refractory metastatic colorectal cancer treated with cetuximab plus bevacizumab. Patients who received cetuximab plus bevacizumab for irinotecan refractory colorectal cancer in either of two Phase II trials conducted were identified. Tumor tissue was available for 33 patients. Genomic DNA was extracted and used for mutational analysis of KRAS, BRAF, and p53 genes. Fluorescence in situ hybridization was performed to assess EGFR copy number. The status of single genes and various combinations were tested for association with response. Seven of 33 patients responded to treatment. KRAS mutations were found in 14/33 cases, and 0 responded to treatment (p = 0.01). EGFR gene amplification was seen in 3/33 of tumors and in every case was associated with response to treatment (p < 0.001). TP53 and BRAF mutations were found in 18/33 and 0/33 tumors, respectively, and there were no associations with response to either gene. EGFR gene amplification and KRAS mutations are predictive markers for patients receiving combination biologic therapy of cetuximab plus bevacizumab for metastatic colorectal cancer. One marker or the other is present in the tumor of half of all patients allowing treatment response to be predicted with a high degree of certainty. The role for molecular markers in combination biologic therapy seems promising.
Keywords: Bevacizumab; Cetuximab; Colorectal cancer; EGFR; KRAS; Metastasis.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Macdonald JS. Adjuvant therapy of colon cancer. CA Cancer J Clin. 1999;49:202–19. - PubMed
-
- Meyerhardt JA, Mayer RJ. Systemic Therapy for Colorectal Cancer. N Engl J Med. 2005;352:476–87. - PubMed
-
- Hicklin DJ, Ellis LM. Role of the Vascular Endothelial Growth Factor Pathway in Tumor Growth and Angiogenesis. J Clin Oncol. 2005;23:1011–27. - PubMed
-
- Cunningham D, Humblet Y, Siena S, et al. Cetuximab Monotherapy and Cetuximab plus Irinotecan in Irinotecan-Refractory Metastatic Colorectal Cancer. N Engl J Med. 2004;351:337–45. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous