

Late Surgical-Site Infection in Immediate Implant-Based Breast Reconstruction
- PMID: 28027221
- PMCID: PMC5675129
- DOI: 10.1097/PRS.0000000000002839
Late Surgical-Site Infection in Immediate Implant-Based Breast Reconstruction
Abstract
Background: Surgical-site infection causes devastating reconstructive failure in implant-based breast reconstructions. Large national database studies offer insights into complication rates, but only capture outcomes within 30 days postoperatively. This study evaluates both early and late surgical-site infection in immediate implant-based reconstruction and identifies predictors.
Methods: As part of the Mastectomy Reconstruction Outcomes Consortium Study, 1662 implant-based breast reconstructions in 1024 patients were evaluated for early versus late surgical-site infection. Early surgical-site infection was defined as infection occurring within 30 days postoperatively; late surgical-site infection was defined as infection occurring 31 days to 1 year postoperatively. Minor infection required oral antibiotics only, and major infection required hospitalization and/or surgical treatment. Direct-to-implant patients had 1-year follow-up, and tissue expander patients had 1-year post-exchange follow-up.
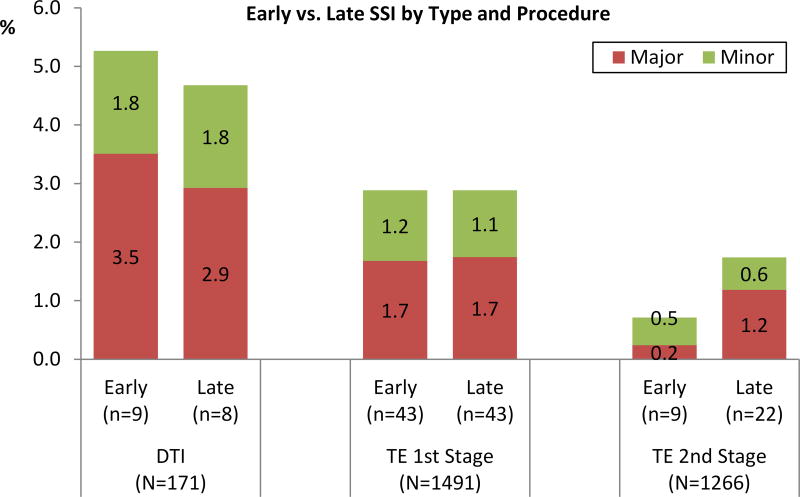
Results: Among 1491 tissue expander and 171 direct-to-implant reconstructions, overall surgical-site infection rate for tissue expander was 5.7 percent (85 of 1491) after first-stage, 2.5 percent (31 of 1266) after second-stage, and 9.9 percent (17 of 171) for direct-to-implant reconstruction. Over 47 to 71 percent of surgical-site infection complications were late surgical-site infection. Multivariate analysis identified radiotherapy and increasing body mass index as significant predictors of late surgical-site infection. No significant difference between the direct-to-implant and tissue expander groups in the occurrence of early, late, or overall surgical-site infection was found.
Conclusions: The majority of surgical-site infection complications in immediate implant-based breast reconstructions occur more than 30 days after both first-stage and second-stage procedures. Radiotherapy and obesity are significantly associated with late-onset surgical-site infection. Current studies limited to early complications do not present a complete assessment of infection associated with implant-based breast reconstructions or their long-term clinical outcomes.
Clinical question/level of evidence: Risk, II.
Conflict of interest statement
Figures
Comment in
-
Reply: Late Surgical-Site Infection in Immediate Implant-Based Breast Reconstruction.Plast Reconstr Surg. 2017 Nov;140(5):750e. doi: 10.1097/PRS.0000000000003778. Plast Reconstr Surg. 2017. PMID: 29068952 No abstract available.
References
-
- Fischer JP, Nelson JA, Serletti JM, Wu JZ. Peri-operative risk factors associated with early tissue expander loss following immediate breast reconstruction: A review of 9305 patients from the 2005–2010 ACS-NSQIP datasets. J Plast Recon Aesthet Surg. 2013;66:15014–12. - PubMed
-
- Albornoz CR, Bach PB, Mehrara BJ, et al. A paradigm shift in US breast reconstruction: increasing implant rates. J Plast Reconstr Surg. 2013;131:15–23. - PubMed
-
- Cemal Y, Albornoz CR, Disa JJ, et al. A paradign shift in US breast reconstruction: part 2. The influence of changing mastectomy patters on reconstructive rate and method. J Plast Reconstr Surg. 2013;131:320e–6e. - PubMed
-
- Argenta LC. Reconstruction of the breast by tissue expansion. Clin Surg. 1984;11:257–64. - PubMed
-
- Shaikh-Naidu N, Preminger B, Rogers K, et al. Determinants of aesthetic satisfaction following TRAM and implant based breast reconstruction. Ann Plast Surg. 2004;52:465–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
