

Association Between Hospital Penalty Status Under the Hospital Readmission Reduction Program and Readmission Rates for Target and Nontarget Conditions
- PMID: 28027367
- PMCID: PMC5599851
- DOI: 10.1001/jama.2016.18533
Association Between Hospital Penalty Status Under the Hospital Readmission Reduction Program and Readmission Rates for Target and Nontarget Conditions
Abstract
Importance: Readmission rates declined after announcement of the Hospital Readmission Reduction Program (HRRP), which penalizes hospitals for excess readmissions for acute myocardial infarction (AMI), heart failure (HF), and pneumonia.
Objective: To compare trends in readmission rates for target and nontarget conditions, stratified by hospital penalty status.
Design, setting, and participants: Retrospective cohort study of Medicare fee-for-service beneficiaries older than 64 years discharged between January 1, 2008, and June 30, 2015, from 2214 penalty hospitals and 1283 nonpenalty hospitals. Difference-interrupted time-series models were used to compare trends in readmission rates by condition and penalty status.
Exposure: Hospital penalty status or target condition under the HRRP.
Main outcomes and measures: Thirty-day risk adjusted, all-cause unplanned readmission rates for target and nontarget conditions.
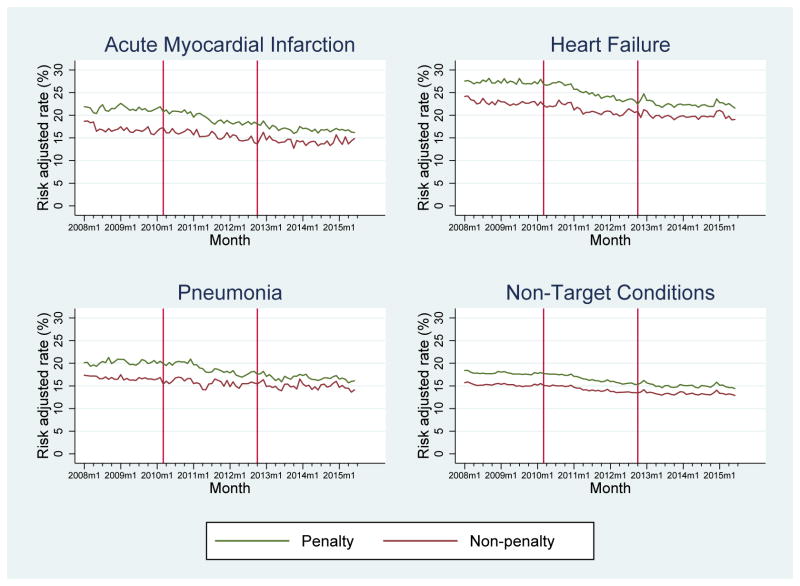
Results: The study included 48 137 102 hospitalizations of 20 351 161 Medicare beneficiaries. In January 2008, the mean readmission rates for AMI, HF, pneumonia, and nontarget conditions were 21.9%, 27.5%, 20.1%, and 18.4%, respectively, at hospitals later subject to financial penalties and 18.7%, 24.2%, 17.4%, and 15.7% at hospitals not subject to penalties. Between January 2008 and March 2010, prior to HRRP announcement, readmission rates were stable across hospitals (except AMI at nonpenalty hospitals). Following announcement of HRRP (March 2010), readmission rates for both target and nontarget conditions declined significantly faster for patients at hospitals later subject to financial penalties compared with those at nonpenalized hospitals (for AMI, additional decrease of -1.24 [95% CI, -1.84 to -0.65] percentage points per year relative to nonpenalty discharges; for HF, -1.25 [95% CI, -1.64 to -0.86]; for pneumonia, -1.37 [95% CI, -1.80 to -0.95]; and for nontarget conditions, -0.27 [95% CI, -0.38 to -0.17]; P < .001 for all). For penalty hospitals, readmission rates for target conditions declined significantly faster compared with nontarget conditions (for AMI, additional decline of -0.49 [95% CI, -0.81 to -0.16] percentage points per year relative to nontarget conditions [P = .004]; for HF, -0.90 [95% CI, -1.18 to -0.62; P < .001]; and for pneumonia, -0.57 [95% CI, -0.92 to -0.23; P < .001]). In contrast, among nonpenalty hospitals, readmissions for target conditions declined similarly or more slowly compared with nontarget conditions (for AMI, additional increase of 0.48 [95% CI, 0.01-0.95] percentage points per year [P = .05]; for HF, 0.08 [95% CI, -0.30 to 0.46; P = .67]; for pneumonia, 0.53 [95% CI, 0.13-0.93; P = .01]). After HRRP implementation in October 2012, the rate of change for readmission rates plateaued (P < .05 for all except pneumonia at nonpenalty hospitals), with the greatest relative change observed among hospitals subject to financial penalty.
Conclusions and relevance: Medicare fee-for-service patients at hospitals subject to penalties under the HRRP had greater reductions in readmission rates compared with those at nonpenalized hospitals. Changes were greater for target vs nontarget conditions for patients at the penalized hospitals but not at the other hospitals.
Conflict of interest statement
Figures
References
-
-
Hospital Readmission Reduction Program, Patient Protection and Affordable Care Act, §3025 (2010).
-
-
- Rau J. Half Of Nation’s Hospitals Fail Again To Escape Medicare’s Readmission Penalties. [Accessed 15 October, 2015];Kaiser Health News. 2015 http://khn.org/news/half-of-nations-hospitals-fail-again-to-escape-medic...
-
- Boccuti C, Casillas G. Aiming for Fewer Hospital U-Turns: The Medicare Hospital Readmission Reduction Program. Kaiser Family Foundation; Jan, 2015. [Accessed 11 May 2016]. Issue Brief. http://kff.org/medicare/issue-brief/aiming-for-fewer-hospital-u-turns-th...
-
- Zuckerman RB, Sheingold SH, Orav EJ, Ruhter J, Epstein AM. Readmissions, Observation, and the Hospital Readmissions Reduction Program. New England Journal of Medicine. 2016;374(16):1543–1551. - PubMed
-
- Lindenauer PK, Normand SL, Drye EE, et al. Development, validation, and results of a measure of 30-day readmission following hospitalization for pneumonia. J Hosp Med. 2011;6(3):142–150. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
