

Incomplete inhibition by eculizumab: mechanistic evidence for residual C5 activity during strong complement activation
- PMID: 28028023
- PMCID: PMC5324716
- DOI: 10.1182/blood-2016-08-732800
Incomplete inhibition by eculizumab: mechanistic evidence for residual C5 activity during strong complement activation
Abstract
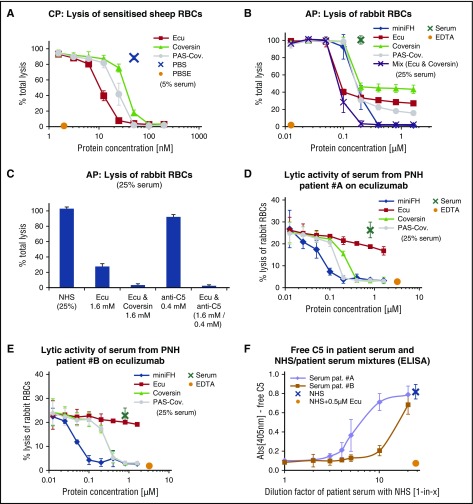
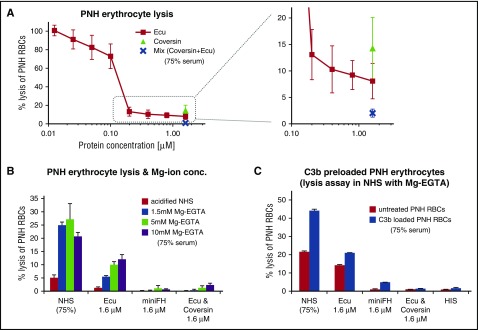
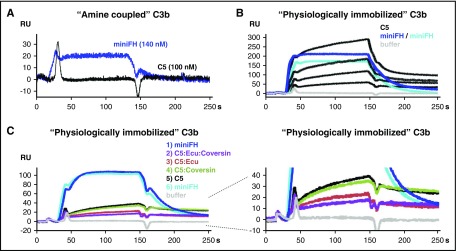
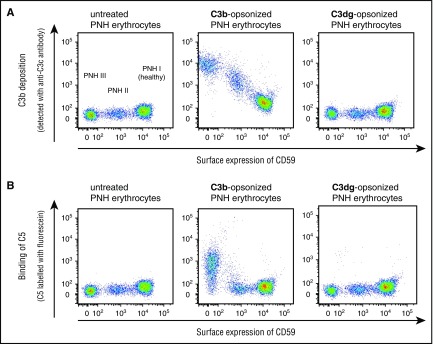
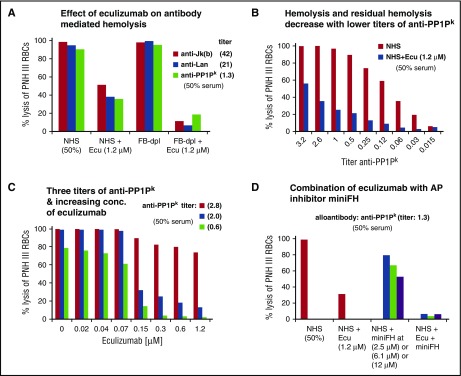
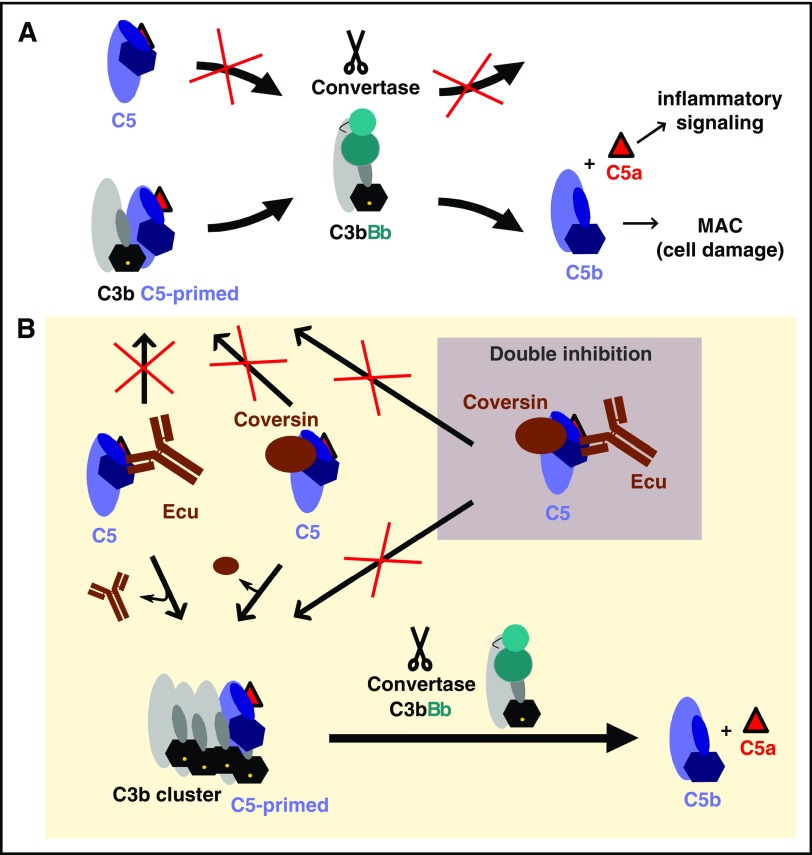
Eculizumab inhibits the terminal, lytic pathway of complement by blocking the activation of the complement protein C5 and shows remarkable clinical benefits in certain complement-mediated diseases. However, several reports suggest that activation of C5 is not always completely suppressed in patients even under excess of eculizumab over C5, indicating that residual C5 activity may derogate the drug's therapeutic benefit under certain conditions. By using eculizumab and the tick-derived C5 inhibitor coversin, we determined conditions ex vivo in which C5 inhibition is incomplete. The degree of such residual lytic activity depended on the strength of the complement activator and the resulting surface density of the complement activation product C3b, which autoamplifies via the alternative pathway (AP) amplification loop. We show that at high C3b densities required for binding and activation of C5, both inhibitors reduce but do not abolish this interaction. The decrease of C5 binding to C3b clusters in the presence of C5 inhibitors correlated with the levels of residual hemolysis. However, by employing different C5 inhibitors simultaneously, residual hemolytic activity could be abolished. The importance of AP-produced C3b clusters for C5 activation in the presence of eculizumab was corroborated by the finding that residual hemolysis after forceful activation of the classical pathway could be reduced by blocking the AP. By providing insights into C5 activation and inhibition, our study delivers the rationale for the clinically observed phenomenon of residual terminal pathway activity under eculizumab treatment with important implications for anti-C5 therapy in general.
© 2017 by The American Society of Hematology.
Figures
Comment in
-
Eculizumab: another breakthrough.Blood. 2017 Feb 23;129(8):922-923. doi: 10.1182/blood-2017-01-760496. Blood. 2017. PMID: 28232621 No abstract available.
References
-
- Hillmen P, Young NS, Schubert J, et al. . The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355(12):1233-1243. - PubMed
-
- Brodsky RA, Young NS, Antonioli E, et al. . Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111(4):1840-1847. - PubMed
-
- Legendre CM, Licht C, Muus P, et al. . Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368(23):2169-2181. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
