

Causes of death in children younger than five years in China in 2015: an updated analysis
- PMID: 28028436
- PMCID: PMC5140075
- DOI: 10.7189/jogh.06.020802
Causes of death in children younger than five years in China in 2015: an updated analysis
Abstract
Background: Substantial progress in reducing the child mortality rate has been made globally in the last two decades. However, for China, the number of children dying from preventable diseases is still very large. It is important to have regularly updated information on the distribution of causes of death (COD) in children to inform policy and research. In this study, we aim to estimate the COD spectrum in children younger than five years old from 2009 to 2015 with a focus on the year 2015 and to provide an updated COD prediction model for China.
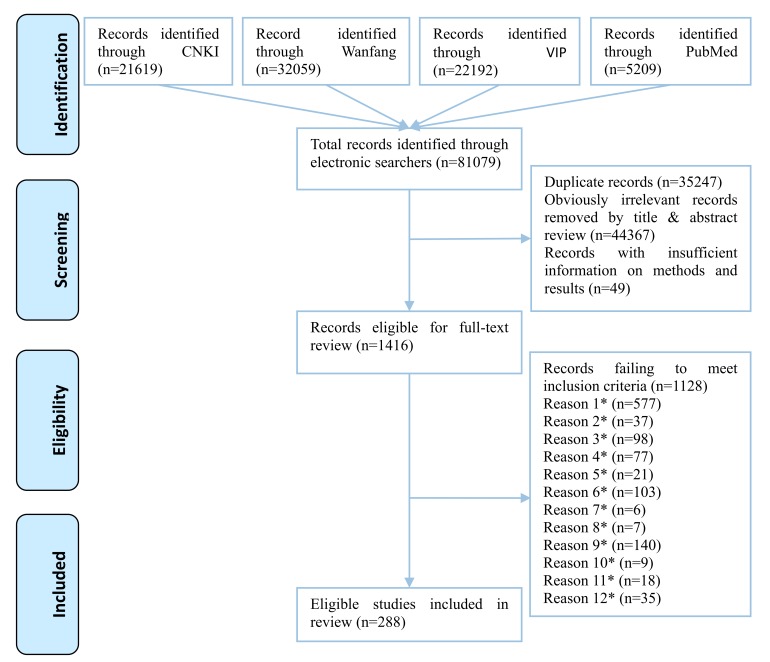
Methods: Updated data of under-five mortality rates (U5MRs) and the number of live births at national and provincial levels were obtained from United Nation's Inter-agency Group for Child Mortality Estimation (UN IGME), Institute for Health Metrics and Evaluation (IHME), and United Nations Population Division (UNPD). Then, we conducted a systematic review across four Chinese and English bibliographic databases and identified high-quality community-based longitudinal studies of COD in children younger than five years in China. We developed a number of single-cause models to predict the number of child death for main COD in different age groups at both national and provincial levels. The jackknife procedure was applied to construct the 95% Uncertainty Ranges (URs).
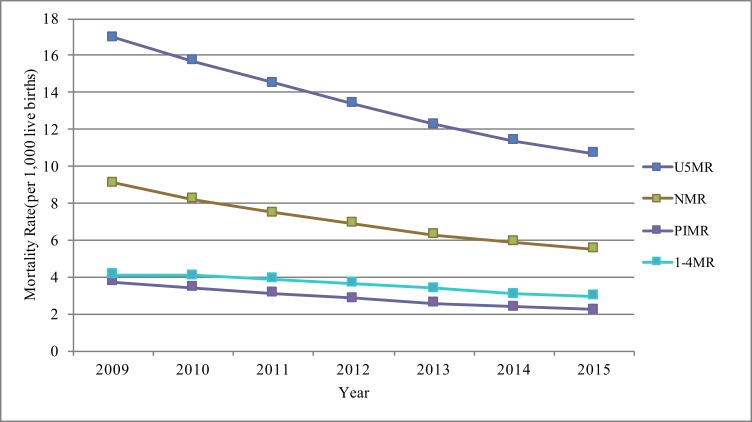
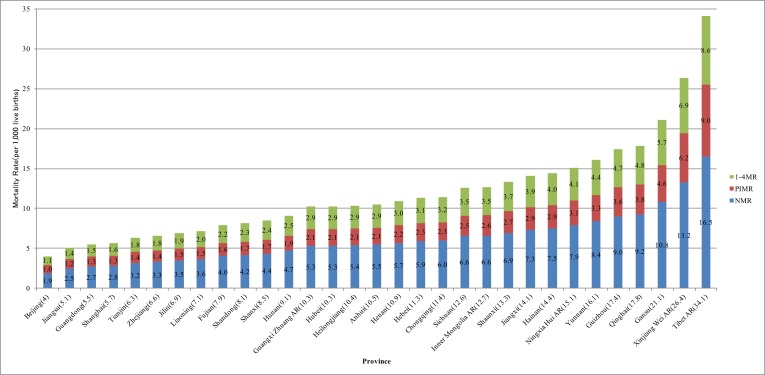
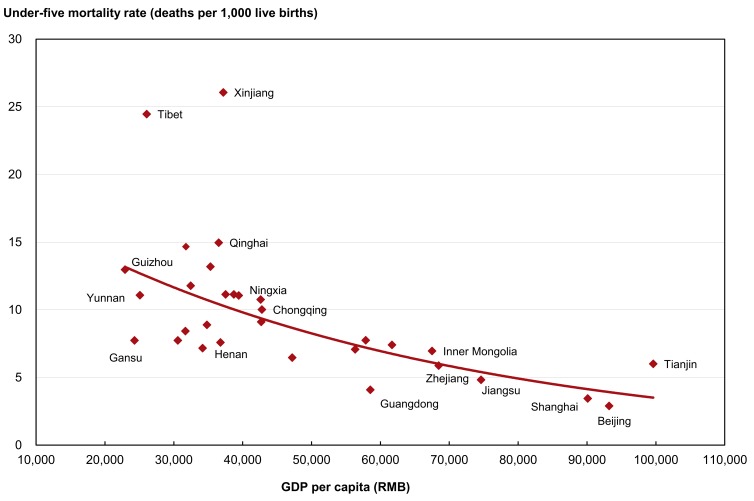
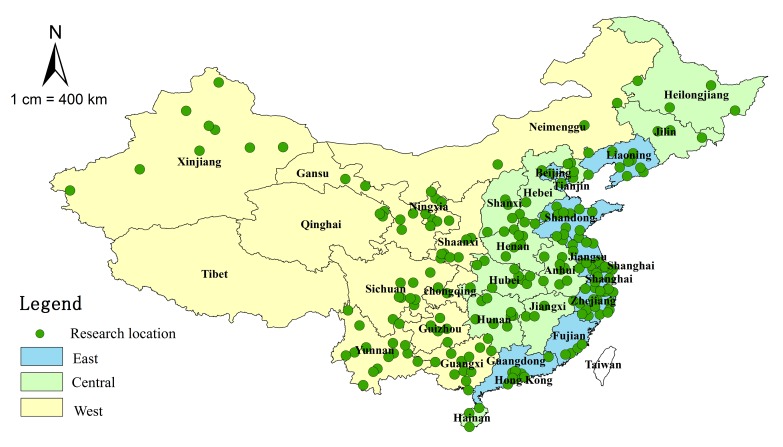
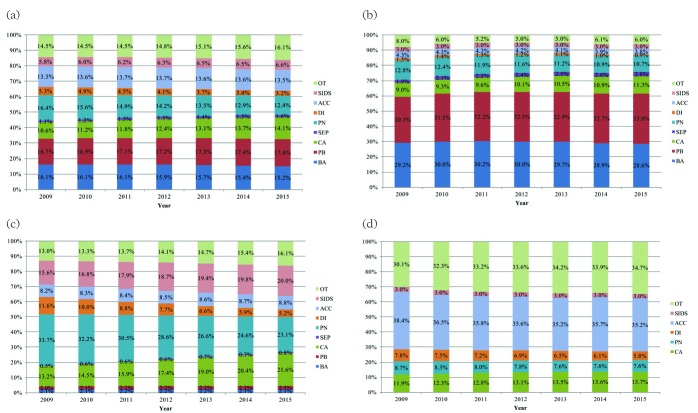
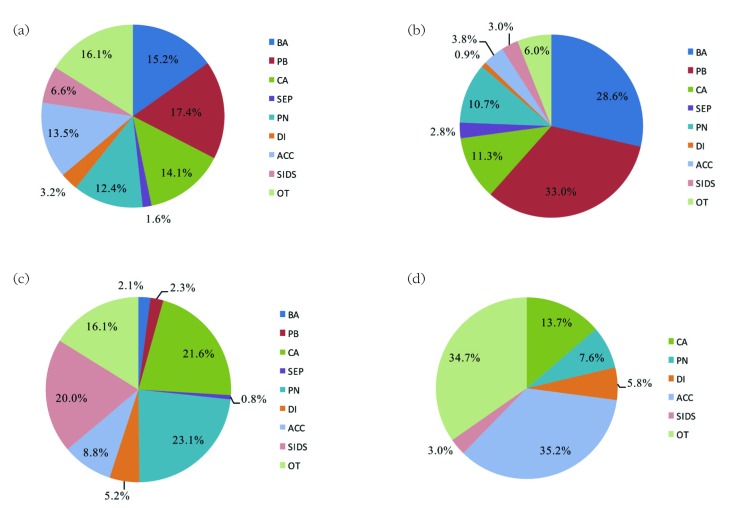
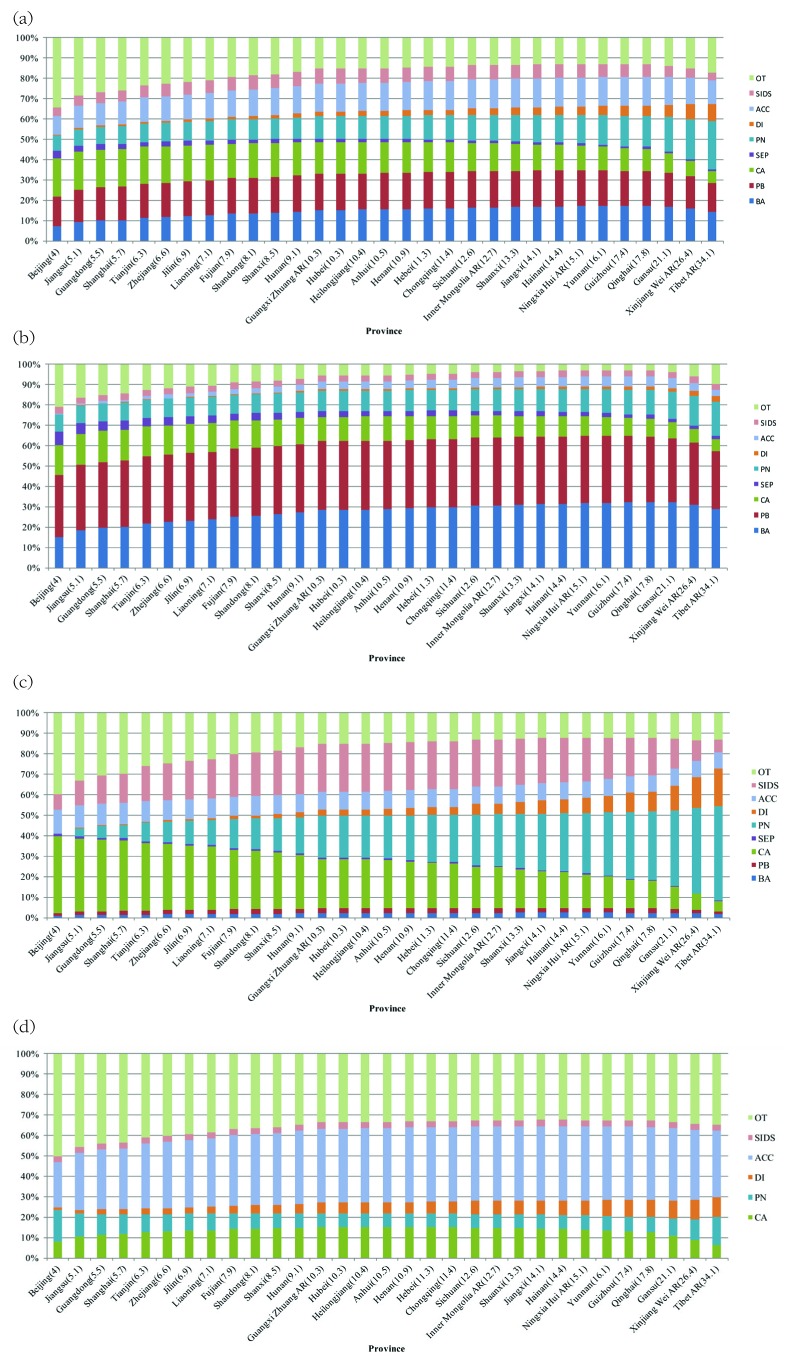
Results: From 2009 to 2015, the under-five mortality rates have declined by 37.1%. The leading causes of death in 2015 were preterm birth complications (17.4%), birth asphyxia (15.2%), congenital abnormalities (14.1%), accidents (13.5%) and pneumonia (12.4%) for children under five years old. The COD spectrum varied substantially across Chinese provinces with different development levels. The leading cause in children under five years in the wealthier provinces (with lower U5MRs) was congenital abnormalities (up to 18.9%), while in the poorer provinces (with higher U5MRs), pneumonia was the dominant COD (up to 23.4%).
Conclusions: This study updates and validates the accuracy of the findings of our previous COD study and proposes a new modelling method to predict proportions for the most common causes of child death in China. These updated COD estimates suggest that current strategies to reduce child mortality should prioritise action on neonatal deaths and target interventions against the top COD according to the local COD spectrum. Special attention should also be given to reducing differences between Chinese provinces and regions with differing development levels.
Figures
References
-
- Currie J, Reichman N. Policies to promote child health: introducing the issue. Future Child. 2015;25:3.
-
- UNICEF. Basic indicators. Available: http://www.unicef.org/infobycountry/stats_popup1.html. Accessed: 2 December 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
