

Prophylactic steroid administration for strictures after endoscopic resection of large superficial esophageal squamous cell carcinoma
- PMID: 28028531
- PMCID: PMC5179327
- DOI: 10.1055/s-0042-118291
Prophylactic steroid administration for strictures after endoscopic resection of large superficial esophageal squamous cell carcinoma
Abstract
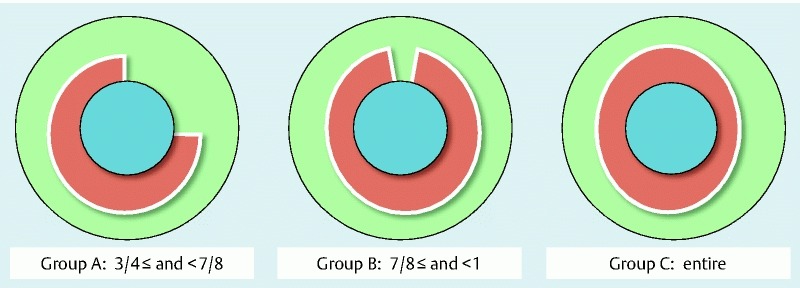
Background and study aims: One of the major complications after endoscopic resection (ER) for large superficial esophageal squamous cell carcinoma (ESCC) is benign esophageal stricture, which can reduce quality of life even if ESCC achieves a cure without organ resection. Recently, steroid administration has been reported as a prophylactic treatment to prevent esophageal strictures. This retrospective study evaluated the stricture rate according to the different width of mucosal defects due to ER and compared it to that seen with prophylactic steroid administration. Patients and methods: Between June 2007 and December 2013, we enrolled patients with ESCC who had 3/4 or larger circumferential mucosal defects due to ER. In December 2009, steroid injections (triamcinolone acetonide 50 mg) into the ulcer bed due to ER were introduced. Beginning in November 2012, we commenced oral steroid administration (prednisolone 30 mg/day, tapered gradually for 8 weeks) in addition to steroid injection. Patients were classified into 3 groups according to the width of mucosal defect after ER (Group A, ≥ 3/4 and < 7/8; Group B, ≥ 7/8 and less than the entire circumference; and Group C, the entire circumference). We retrospectively evaluated the stricture rate by comparing no treatment, steroid injection, or steroid injection followed by oral steroid according to the width of mucosal defect. Results: A total of 115 patients met the selection criteria. In Group B, no treatment had a significantly higher stricture rate (100 %, vs. steroid injection: 56 % P = 0.015; vs steroid injection followed by oral steroid: 20 % P < 0.001). Conversely, in Group C, the stricture rate was high, regardless of treatment (no treatment: 100 %; steroid injection: 100 %; steroid injection followed by oral steroid: 71 %). Conclusions: Although prophylactic steroid administration is effective to prevent strictures for 7/8 circumference or larger mucosal defects, it is ineffective for whole-circumference defects. Further investigation is required.
Conflict of interest statement
Figures
References
-
- Oyama T, Tomori A, Hotta K. et al.Endoscopic submucosal dissection of early esophageal cancer. Clin Gastroenterol Hepatol. 2005;3:67–70. - PubMed
-
- Ono S, Fujishiro M, Niimi K. et al.Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest Endosc. 2009;70:860–866. - PubMed
-
- Mizuta H, Nishimori I, Kuratani Y. et al.Predictive factors for esophageal stenosis after endoscopic submucosal dissection for superficial esophageal cancer. Dis Esophagus. 2009;22:626–631. - PubMed
-
- Ono S, Fujishiro M, Niimi K. et al.Predictors of postoperative stricture after esophageal endoscopic submucosal dissection for superficial squamous cell neoplasms. Endoscopy. 2009;41:661–665. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous