

Impact of histological subtype on survival in patients with locally advanced cervical cancer that were treated with definitive radiotherapy: adenocarcinoma/adenosquamous carcinoma versus squamous cell carcinoma
- PMID: 28028992
- PMCID: PMC5323286
- DOI: 10.3802/jgo.2017.28.e19
Impact of histological subtype on survival in patients with locally advanced cervical cancer that were treated with definitive radiotherapy: adenocarcinoma/adenosquamous carcinoma versus squamous cell carcinoma
Abstract
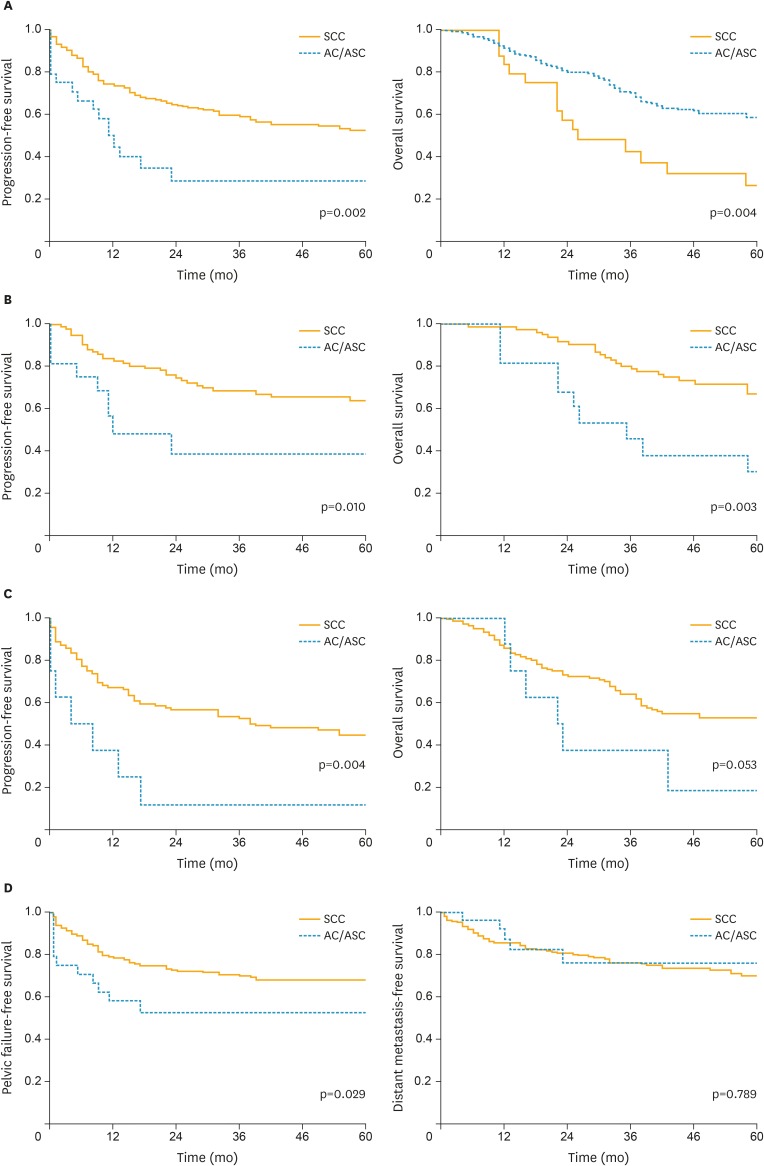
Objective: To compare the survival outcomes of patients with cervical squamous cell carcinoma (SCC) and adenocarcinoma/adenosquamous carcinoma (AC/ASC) among patients with locally advanced cervical cancer that were treated with definitive radiotherapy.
Methods: The baseline characteristics and outcome data of patients with locally advanced cervical cancer who were treated with definitive radiotherapy between November 1993 and February 2014 were collected and retrospectively reviewed. A Cox proportional hazards regression model was used to investigate the prognostic significance of AC/ASC histology.
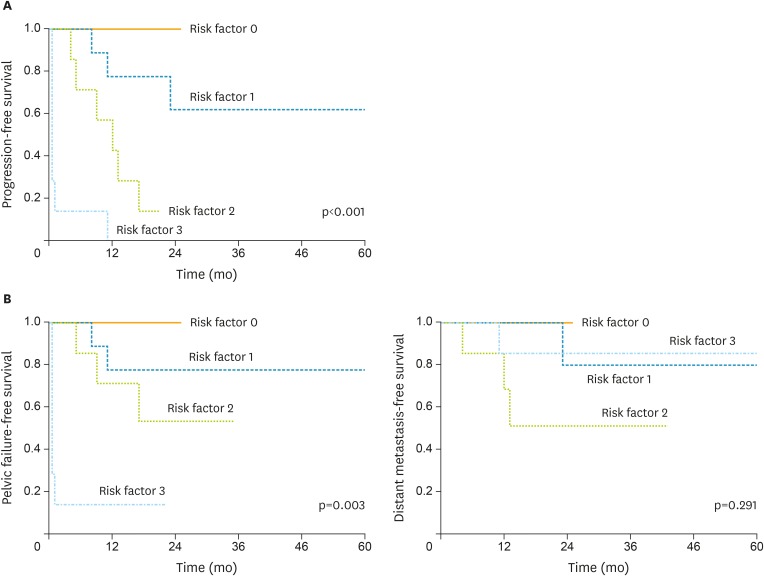
Results: The patients with AC/ASC of the cervix exhibited significantly shorter overall survival (OS) (p=0.004) and progression-free survival (PFS) (p=0.002) than the patients with SCC of the cervix. Multivariate analysis showed that AC/ASC histology was an independent negative prognostic factor for PFS. Among the patients who displayed AC/ASC histology, larger tumor size, older age, and incomplete response to radiotherapy were found to be independent prognostic factors. PFS was inversely associated with the number of poor prognostic factors the patients exhibited (the estimated 1-year PFS rates; 100.0%, 77.8%, 42.8%, 0.0% for 0, 1, 2, 3 factors, respectively).
Conclusion: Locally advanced cervical cancer patients with AC/ASC histology experience significantly worse survival outcomes than those with SCC. Further clinical studies are warranted to develop a concurrent chemoradiotherapy (CCRT) protocol that is specifically tailored to locally advanced cervical AC/ASC.
Keywords: Adenocarcinoma; Carcinoma, Adenosquamous; Radiotherapy; Uterine Cervical Neoplasms.
Copyright © 2017. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Wang SS, Sherman ME, Hildesheim A, Lacey JV, Jr, Devesa S. Cervical adenocarcinoma and squamous cell carcinoma incidence trends among white women and black women in the United States for 1976–2000. Cancer. 2004;100:1035–1044. - PubMed
-
- Bray F, Carstensen B, Møller H, Zappa M, Zakelj MP, Lawrence G, et al. Incidence trends of adenocarcinoma of the cervix in 13 European countries. Cancer Epidemiol Biomarkers Prev. 2005;14:2191–2199. - PubMed
-
- Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med. 1999;340:1137–1143. - PubMed
-
- Keys HM, Bundy BN, Stehman FB, Muderspach LI, Chafe WE, Suggs CL, 3rd, et al. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl J Med. 1999;340:1154–1161. - PubMed
-
- Rose PG, Bundy BN, Watkins EB, Thigpen JT, Deppe G, Maiman MA, et al. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N Engl J Med. 1999;340:1144–1153. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
