

Hemodynamic mechanisms underlying elevated oxygen extraction fraction (OEF) in moyamoya and sickle cell anemia patients
- PMID: 28029271
- PMCID: PMC6125968
- DOI: 10.1177/0271678X16682509
Hemodynamic mechanisms underlying elevated oxygen extraction fraction (OEF) in moyamoya and sickle cell anemia patients
Abstract
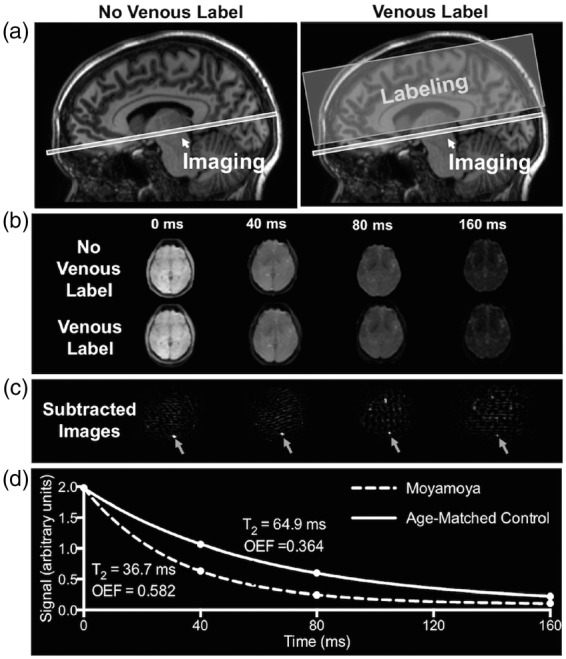
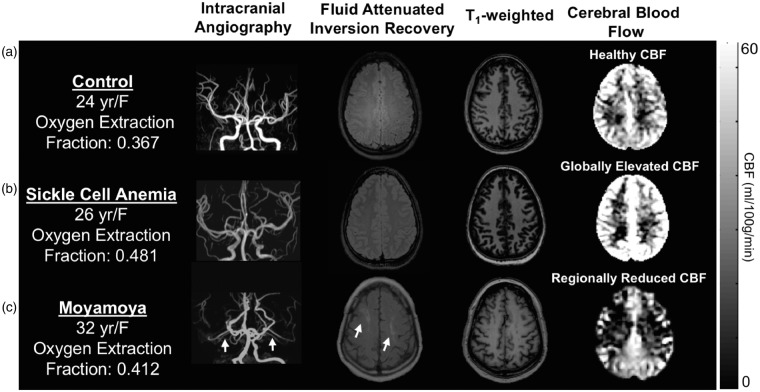
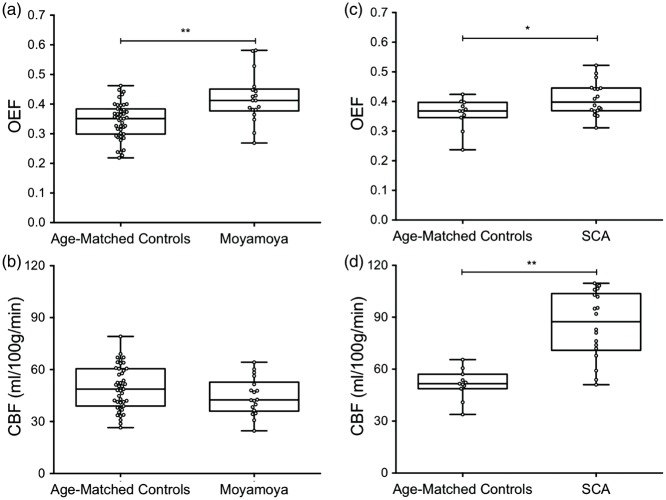
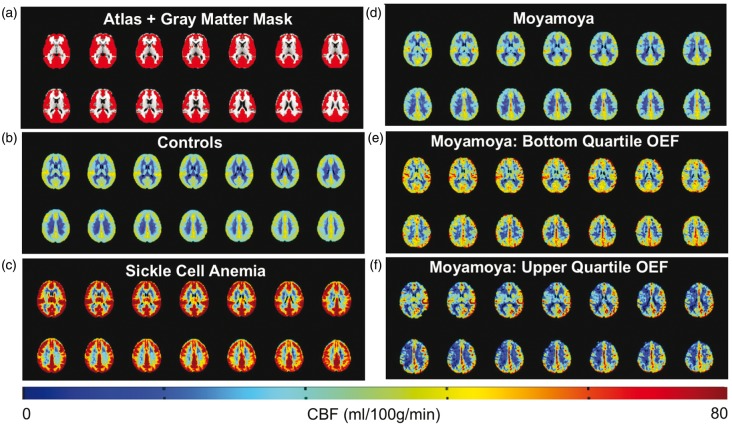
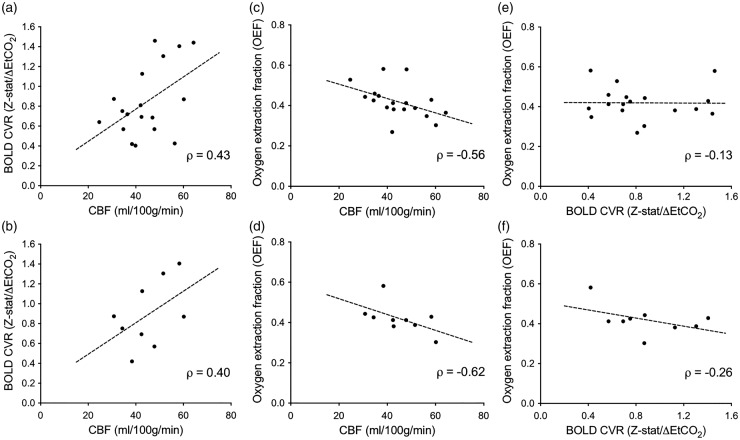
Moyamoya is a bilateral, complex cerebrovascular condition characterized by progressive non-atherosclerotic intracranial stenosis and collateral vessel formation. Moyamoya treatment focuses on restoring cerebral blood flow (CBF) through surgical revascularization, however stratifying patients for revascularization requires abilities to quantify how well parenchyma is compensating for arterial steno-occlusion. Globally elevated oxygen extraction fraction (OEF) secondary to CBF reduction may serve as a biomarker for tissue health in moyamoya patients, as suggested in patients with sickle cell anemia (SCA) and reduced oxygen carrying capacity. Here, OEF was measured (TRUST-MRI) to test the hypothesis that OEF is globally elevated in patients with moyamoya (n = 18) and SCA (n = 18) relative to age-matched controls (n = 43). Mechanisms underlying the hypothesized OEF increases were evaluated by performing sequential CBF-weighted, cerebrovascular reactivity (CVR)-weighted, and structural MRI. Patients were stratified by treatment and non-parametric tests applied to compare study variables (significance: two-sided P < 0.05). OEF was significantly elevated in moyamoya participants (interquartile range = 0.38-0.45) compared to controls (interquartile range = 0.29-0.38), similar to participants with SCA (interquartile range = 0.37-0.45). CBF was inversely correlated with OEF in moyamoya participants. Elevated OEF was only weakly related to reductions in CVR, consistent with basal CBF level, rather than vascular reserve capacity, being most closely associated with OEF.
Keywords: MRI; Oxygen extraction fraction; moyamoya; neurophysiology; stroke.
Figures
References
-
- Scott RM, Smith ER. Moyamoya disease and moyamoya syndrome. New Engl J Med 2009; 360: 1226–1237. - PubMed
-
- Hallemeier CL, Rich KM, Grubb RL, Jr., et al. Clinical features and outcome in North American adults with moyamoya phenomenon. Stroke 2006; 37: 1490–1496. - PubMed
-
- Arias EJ, Derdeyn CP, Dacey RG, Jr., et al. Advances and surgical considerations in the treatment of moyamoya disease. Neurosurgery 2014; 74(Suppl 1): S116–S125. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
