

Impact of Examined Lymph Node Count on Precise Staging and Long-Term Survival of Resected Non-Small-Cell Lung Cancer: A Population Study of the US SEER Database and a Chinese Multi-Institutional Registry
- PMID: 28029318
- PMCID: PMC5455598
- DOI: 10.1200/JCO.2016.67.5140
Impact of Examined Lymph Node Count on Precise Staging and Long-Term Survival of Resected Non-Small-Cell Lung Cancer: A Population Study of the US SEER Database and a Chinese Multi-Institutional Registry
Abstract
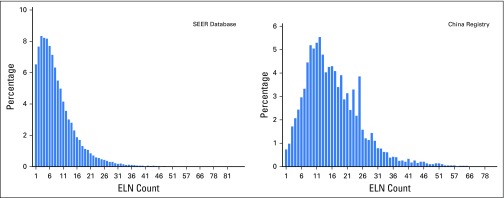
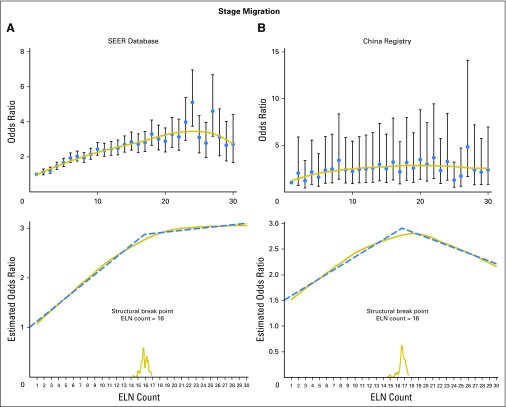
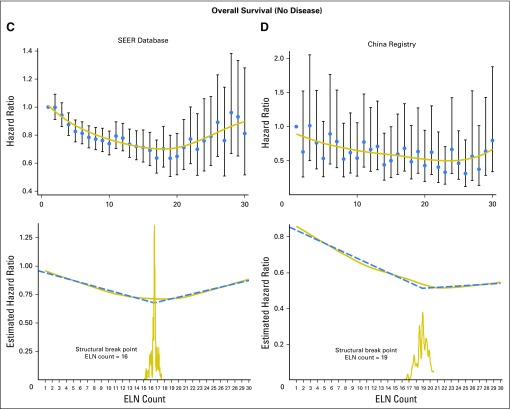
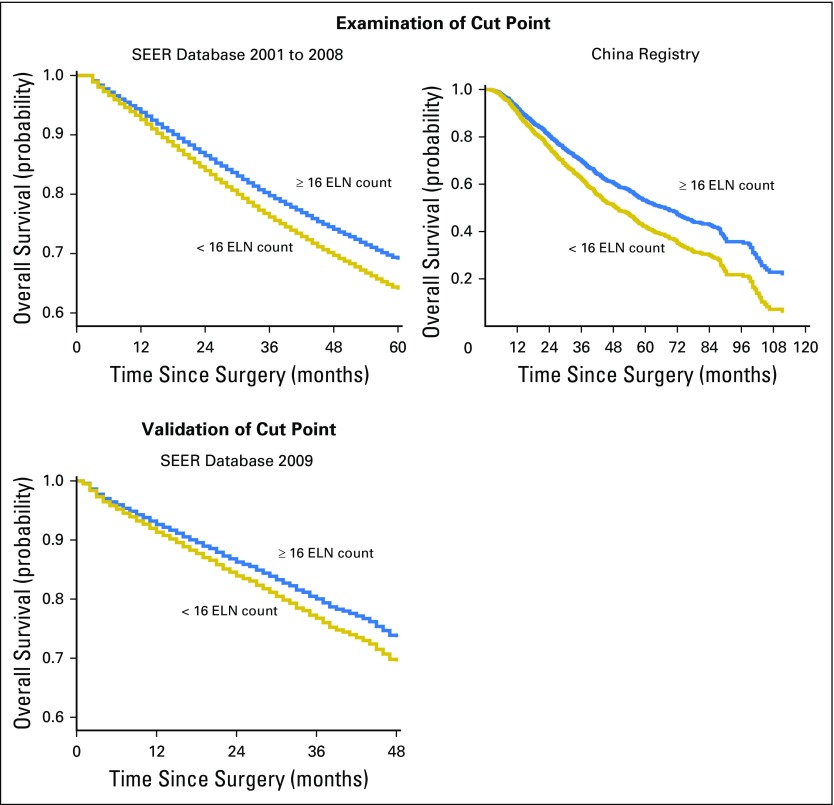
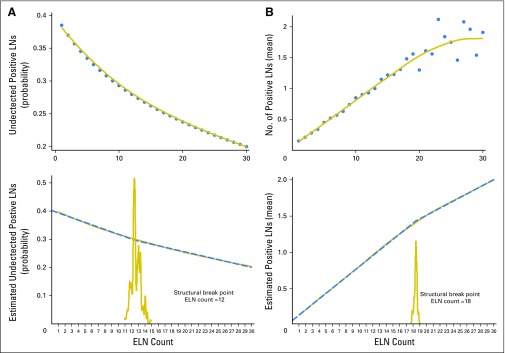
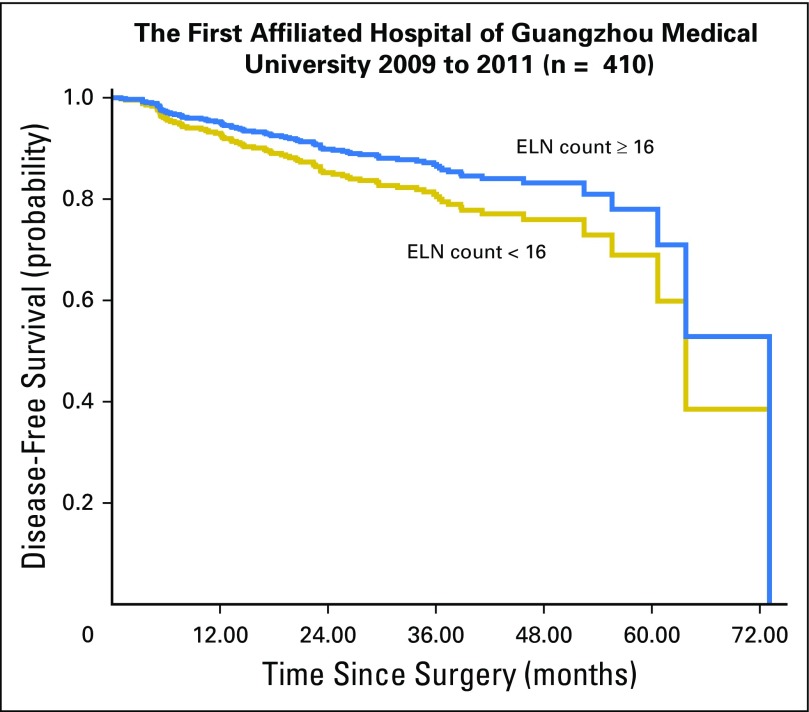
Purpose We investigated the correlation between the number of examined lymph nodes (ELNs) and correct staging and long-term survival in non-small-cell lung cancer (NSCLC) by using large databases and determined the minimal threshold for the ELN count. Methods Data from a Chinese multi-institutional registry and the US SEER database on stage I to IIIA resected NSCLC (2001 to 2008) were analyzed for the relationship between the ELN count and stage migration and overall survival (OS) by using multivariable models. The series of the mean positive LNs, odds ratios (ORs), and hazard ratios (HRs) were fitted with a LOWESS smoother, and the structural break points were determined by Chow test. The selected cut point was validated with the SEER 2009 cohort. Results Although the distribution of ELN count differed between the Chinese registry (n = 5,706) and the SEER database (n = 38,806; median, 15 versus seven, respectively), both cohorts exhibited significantly proportional increases from N0 to N1 and N2 disease (SEER OR, 1.038; China OR, 1.012; both P < .001) and serial improvements in OS (N0 disease: SEER HR, 0.986; China HR, 0.981; both P < .001; N1 and N2 disease: SEER HR, 0.989; China HR, 0.984; both P < .001) as the ELN count increased after controlling for confounders. Cut point analysis showed a threshold ELN count of 16 in patients with declared node-negative disease, which were examined in the derivation cohorts (SEER 2001 to 2008 HR, 0.830; China HR, 0.738) and validated in the SEER 2009 cohort (HR, 0.837). Conclusion A greater number of ELNs is associated with more-accurate node staging and better long-term survival of resected NSCLC. We recommend 16 ELNs as the cut point for evaluating the quality of LN examination or prognostic stratification postoperatively for patients with declared node-negative disease.
Figures
Comment in
-
Numbers or Stations: From Systematic Sampling to Individualized Lymph Node Dissection in Non-Small-Cell Lung Cancer.J Clin Oncol. 2017 Apr 10;35(11):1143-1145. doi: 10.1200/JCO.2016.71.8544. Epub 2017 Mar 6. J Clin Oncol. 2017. PMID: 28380312 No abstract available.
-
Examined lymph node count in non-small-cell lung cancer: will it be a decision making approach in treatment of NSCLC?J Thorac Dis. 2017 May;9(5):E480-E482. doi: 10.21037/jtd.2017.03.79. J Thorac Dis. 2017. PMID: 28616315 Free PMC article. No abstract available.
-
Nichtkleinzelliges Bronchialkarzinom: mindestens 16 Lymphknoten entfernen.Zentralbl Chir. 2018 Feb;143(1):16. doi: 10.1055/s-0043-124400. Epub 2018 Feb 26. Zentralbl Chir. 2018. PMID: 29482235 German. No abstract available.
References
-
- Jemal A, Center MM, DeSantis C, et al. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev. 2010;19:1893–1907. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:706–714. - PubMed
-
- National Comprehensive Cancer Network: NCCN clinical practice guidelines in oncology: Non-small cell lung cancer, V.2.2013. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf.
-
- Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552–3559. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
