

Perioperative Major Adverse Cardiovascular and Cerebrovascular Events Associated With Noncardiac Surgery
- PMID: 28030663
- PMCID: PMC5563847
- DOI: 10.1001/jamacardio.2016.4792
Perioperative Major Adverse Cardiovascular and Cerebrovascular Events Associated With Noncardiac Surgery
Abstract
Importance: Major adverse cardiovascular and cerebrovascular events (MACCE) are a significant source of perioperative morbidity and mortality following noncardiac surgery.
Objective: To evaluate national trends in perioperative cardiovascular outcomes and mortality after major noncardiac surgery and to identify surgical subtypes associated with cardiovascular events using a large administrative database of United States hospital admissions.
Design, setting, participants: Patients who underwent major noncardiac surgery from January 2004 to December 2013 were identified using the National Inpatient Sample.
Main outcomes and measures: Perioperative MACCE (primary outcome), defined as in-hospital, all-cause death, acute myocardial infarction (AMI), or acute ischemic stroke, were evaluated over time.
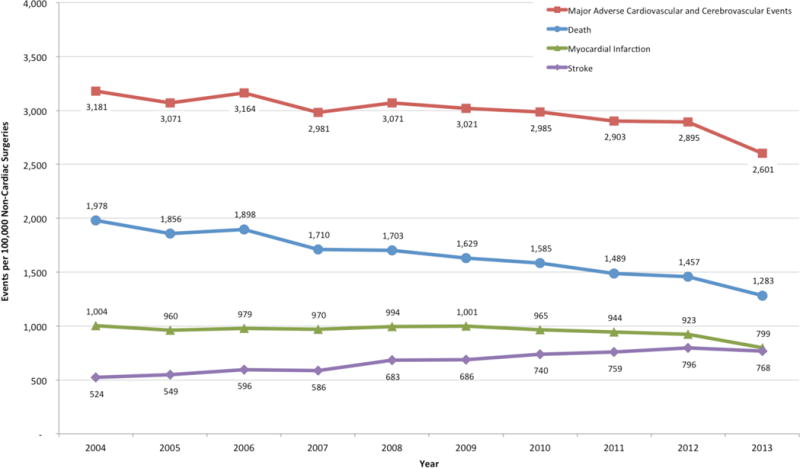
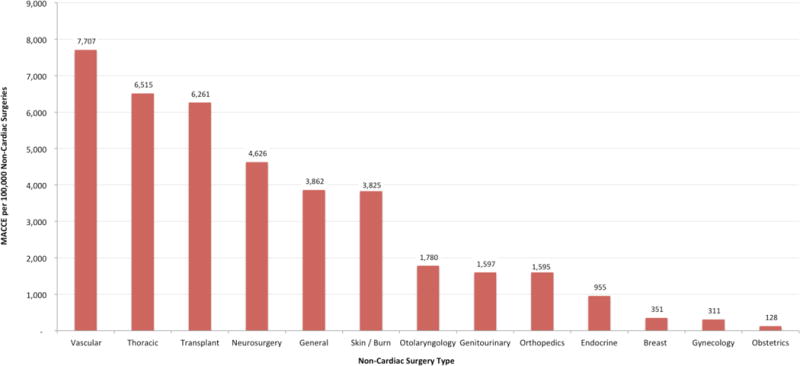
Results: Among 10 581 621 hospitalizations (mean [SD] patient age, 65.74 [12.32] years; 5 975 798 female patients 56.60%]) for major noncardiac surgery, perioperative MACCE occurred in 317 479 hospitalizations (3.0%), corresponding to an annual incidence of approximately 150 000 events after applying sample weights. Major adverse cardiovascular and cerebrovascular events occurred most frequently in patients undergoing vascular (7.7%), thoracic (6.5%), and transplant surgery (6.3%). Between 2004 and 2013, the frequency of MACCE declined from 3.1% to 2.6% (P for trend <.001; adjusted odds ratio [aOR], 0.95; 95% CI, 0.94-0.97) driven by a decline in frequency of perioperative death (aOR, 0.79; 95% CI, 0.77-0.81) and AMI (aOR, 0.87; 95% CI, 0.84-0.89) but an increase in perioperative ischemic stroke from 0.52% in 2004 to 0.77% in 2013 (P for trend <.001; aOR 1.79; CI 1.73-1.86).
Conclusions and relevance: Perioperative MACCE occurs in 1 of every 33 hospitalizations for noncardiac surgery. Despite reductions in the rate of death and AMI among patients undergoing major noncardiac surgery in the United States, perioperative ischemic stroke increased over time. Additional efforts are necessary to improve cardiovascular care in the perioperative period of patients undergoing noncardiac surgery.
Conflict of interest statement
Figures
Comment in
-
Trends in Perioperative Cardiovascular Events: Mostly Sunny, With Showers.JAMA Cardiol. 2017 Feb 1;2(2):188-189. doi: 10.1001/jamacardio.2016.4786. JAMA Cardiol. 2017. PMID: 28030654 No abstract available.
References
-
- Weiser TG, Haynes AB, Molina G, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015 Apr 27;385(Suppl 2):S11. - PubMed
-
- Devereaux PJ, Sessler DI. Cardiac Complications in Patients Undergoing Major Noncardiac Surgery. N Engl J Med. 2015 Dec 3;373(23):2258–2269. - PubMed
-
- Vascular Events In Noncardiac Surgery Patients Cohort Evaluation Study I. Devereaux PJ, Chan MT, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012 Jun 6;307(21):2295–2304. - PubMed
-
- Semel ME, Lipsitz SR, Funk LM, Bader AM, Weiser TG, Gawande AA. Rates and patterns of death after surgery in the United States, 1996 and 2006. Surgery. 2012 Feb;151(2):171–182. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
