

Prognostic factors and failure patterns in non-metastatic nasopharyngeal carcinoma after intensity-modulated radiotherapy
- PMID: 28031050
- PMCID: PMC5192583
- DOI: 10.1186/s40880-016-0167-2
Prognostic factors and failure patterns in non-metastatic nasopharyngeal carcinoma after intensity-modulated radiotherapy
Abstract
Background: The prognostic values of staging parameters require continual re-assessment amid changes in diagnostic and therapeutic methods. This study aimed to identify the prognostic factors and failure patterns of non-metastatic nasopharyngeal carcinoma (NPC) in the intensity-modulated radiotherapy (IMRT) era.
Methods: We reviewed the data from 749 patients with newly diagnosed, biopsy-proven, non-metastatic NPC in our cancer center (South China, an NPC endemic area) between January 2003 and December 2007. All patients underwent magnetic resonance imaging (MRI) before receiving IMRT. The actuarial survival rates were estimated using the Kaplan-Meier method, and survival curves were compared using the log-rank test. Multivariate analyses with the Cox proportional hazards model were used to test for the independent prognostic factors by backward eliminating insignificant explanatory variables.
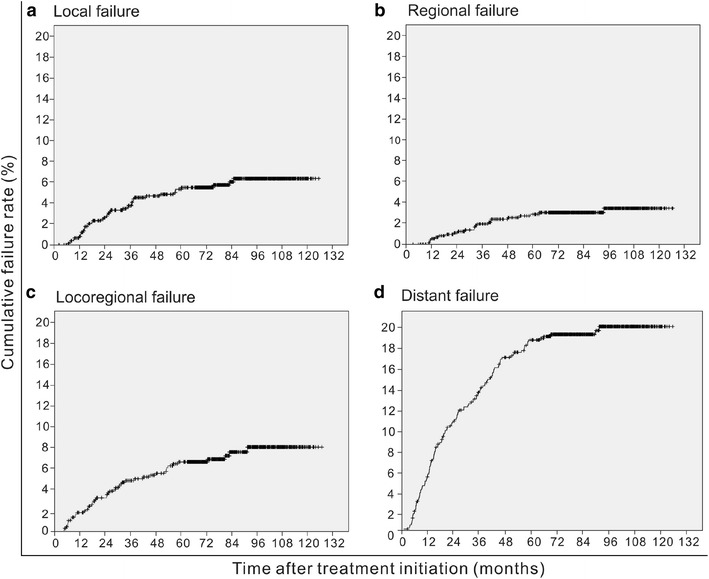
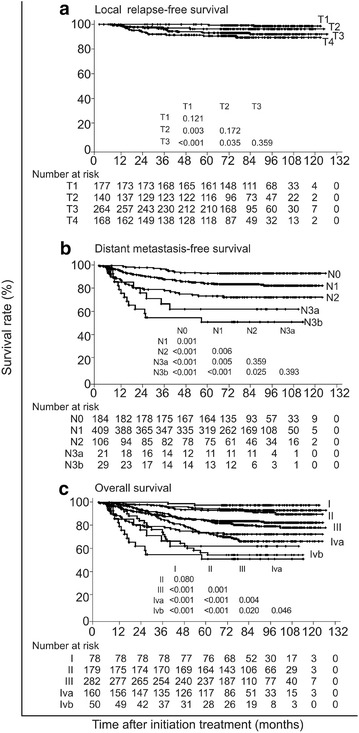
Results: The 5-year occurrence rates of local failure, regional failure, locoregional failure, and distant failure were 5.4, 3.0, 7.4, and 17.4%, respectively. The 5-year survival rates were as follows: local relapse-free survival, 94.6%; nodal relapse-free survival, 97.0%; distant metastasis-free survival, 82.6%; disease-free survival, 75.1%; and overall survival, 82.0%. Multivariate Cox regression analysis revealed that orbit involvement was the only significant prognostic factor for local failure (P = 0.011). Parapharyngeal tumor extension, retropharyngeal lymph node involvement, and the laterality, longest diameter, and Ho's location of the cervical lymph nodes were significant prognostic factors for both distant failure and disease failure (all P < 0.05). Intracranial extension had significant prognostic value for distant failure (P = 0.040).
Conclusions: The key failure pattern for NPC was distant metastasis in the IMRT era. With changes in diagnostic and therapeutic technologies as well as treatment modalities, the significant prognostic parameters for local control have also been altered substantially.
Keywords: Failure pattern; Intensity-modulated radiotherapy; Nasopharyngeal carcinoma; Prognosis; Tumor staging.
Figures
References
-
- Gibb AG, Van Hasselt CA. Nasopharyngeal carcinoma, vol xvii. Hong Kong: Chinese University Press; Greenwich Medical Media; 1999. p. 337.
-
- Moss WT. Therapeutic radiology: rationale, technique, results, vol xviii. St. Louis: C.V. Mosby Co; 1965. p. 514.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
