

Improvement in 5-year mortality in incident rheumatoid arthritis compared with the general population-closing the mortality gap
- PMID: 28031164
- PMCID: PMC5526676
- DOI: 10.1136/annrheumdis-2016-209562
Improvement in 5-year mortality in incident rheumatoid arthritis compared with the general population-closing the mortality gap
Abstract
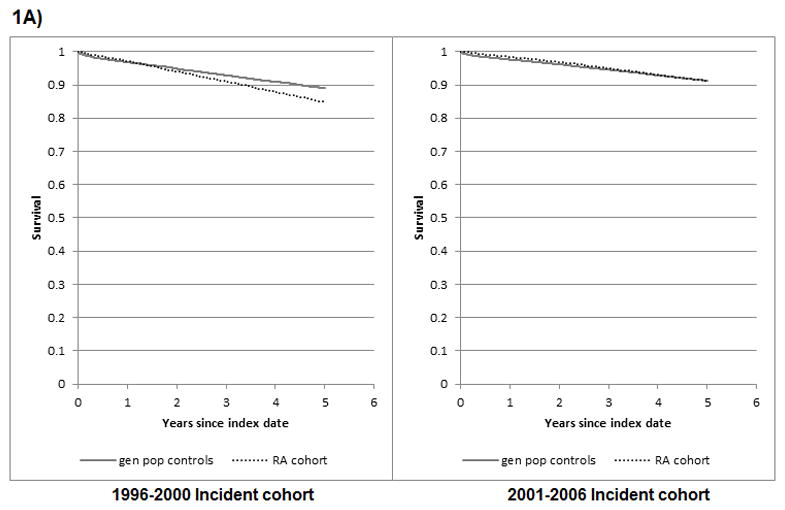
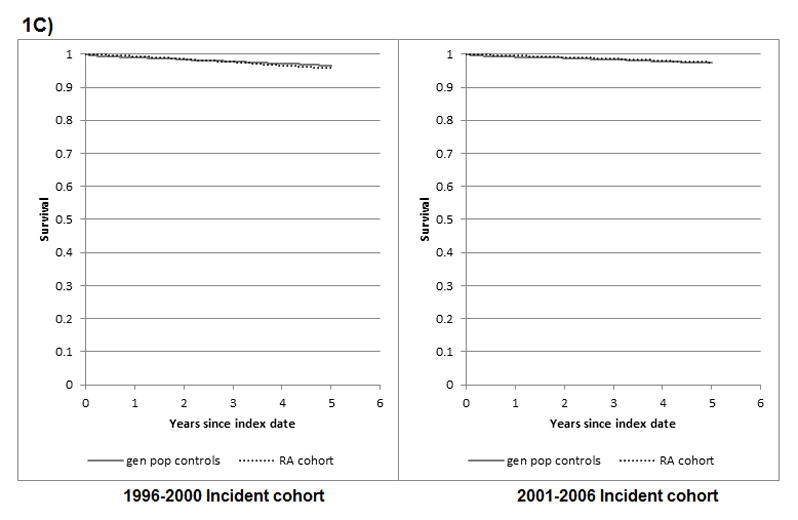
Objective: Excess mortality in rheumatoid arthritis (RA) is expected to have improved over time, due to improved treatment. Our objective was to evaluate secular 5-year mortality trends in RA relative to general population controls in incident RA cohorts diagnosed in 1996-2000 vs 2001-2006.
Methods: We conducted a population-based cohort study, using administrative health data, of all incident RA cases in British Columbia who first met RA criteria between January 1996 and December 2006, with general population controls matched 1:1 on gender, birth and index years. Cohorts were divided into earlier (RA onset 1996-2000) and later (2001-2006) cohorts. Physician visits and vital statistics data were obtained until December 2010. Follow-up was censored at 5 years to ensure equal follow-up in both cohorts. Mortality rates, mortality rate ratios and HRs for mortality (RA vs controls) using proportional hazard models adjusting for age, were calculated. Differences in mortality in RA versus controls between earlier and later incident cohorts were tested via interaction between RA status (case/control) and cohort (earlier/later).
Results: 24 914 RA cases and controls experienced 2747 and 2332 deaths, respectively. Mortality risk in RA versus controls differed across incident cohorts for all-cause, cardiovascular diseases (CVD) and cancer mortality (interactions p<0.01). A significant increase in mortality in RA versus controls was observed in earlier, but not later, cohorts (all-cause mortality adjusted HR (95% CI): 1.40 (1.30 to 1.51) and 0.97 (0.89 to 1.05), respectively).
Conclusions: In our population-based incident RA cohort, mortality compared with the general population improved over time. Increased mortality in the first 5 years was observed in people with RA onset before, but not after, 2000.
Keywords: Epidemiology; Outcomes research; Rheumatoid Arthritis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Cobb S, Anderson F, Bauer W. Length of life and cause of death in rheumatoid arthritis. N Engl J Med. 1953;249:553–6. - PubMed
-
- Naz SM, Symmons DPM. Mortality in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2007;21:871–83. - PubMed
-
- Dadoun Z-KN, Combescure C, Elhai M, Rozenberg S, Gossec L, Fautrel B. Mortality in rheumatoid arthritis over the last fifty years: Systematic review and meta-analysis. Joint Bone Spine. 2013;80:29–33. - PubMed
-
- Myasoedova E, Davis JM, III, Crowson CS, Gabriel SE. Epidemiology of Rheumatoid Arthritis: Rheumatoid Arthritis and Mortality. Curr Rheumatol Rep. 2010;12:379–85. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
