

Overweight and obese but not normal weight women with PCOS are at increased risk of Type 2 diabetes mellitus-a prospective, population-based cohort study
- PMID: 28031324
- PMCID: PMC5260860
- DOI: 10.1093/humrep/dew329
Overweight and obese but not normal weight women with PCOS are at increased risk of Type 2 diabetes mellitus-a prospective, population-based cohort study
Erratum in
-
Overweight and obese but not normal weight women with PCOS are at increased risk of Type 2 diabetes mellitus-a prospective population-based cohort study.Hum Reprod. 2017 Apr 1;32(4):968. doi: 10.1093/humrep/dex030. Hum Reprod. 2017. PMID: 28333219 Free PMC article. No abstract available.
Abstract
Study question: What are the respective roles of polycystic ovary syndrome (PCOS), long-term weight gain and obesity for the development of prediabetes or Type 2 diabetes mellitus (T2DM) by age 46 years?
Summary answer: The risk of T2DM in women with PCOS is mainly due to overweight and obesity, although these two factors have a synergistic effect on the development of T2DM.
What is known already: PCOS is associated with an increased risk of prediabetes and T2DM. However, the respective roles of PCOS per se and BMI for the development of T2DM have remained unclear.
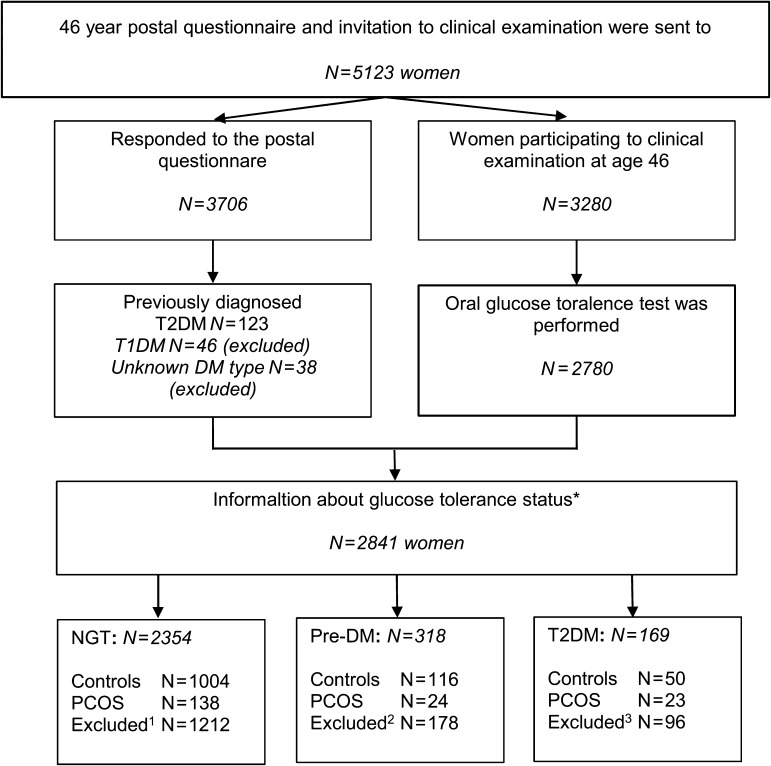
Study design, size, duration: In a prospective, general population-based follow-up birth cohort 1966 (n = 5889), postal questionnaires were sent at ages 14 (95% answered), 31 (80% answered) and 46 years (72% answered). Questions about oligoamenorrhoea and hirsutism were asked at age 31 years, and a question about PCOS diagnosis at 46 years. Clinical examination and blood sampling were performed at 31 years in 3127 women, and at 46 years in 3280 women. A 2-h oral glucose tolerance test (OGTT) was performed at 46 years of age in 2780 women.
Participants/materials, setting, methods: Women reporting both oligoamenorrhoea and hirsutism at age 31 years and/or diagnosis of PCOS by 46 years were considered as women with PCOS (n = 279). Women without any symptoms at 31 years and without PCOS diagnosis by 46 years were considered as controls (n = 1577). The level of glucose metabolism was classified according to the results of the OGTT and previous information of glucose metabolism status from the national drug and hospital discharge registers.
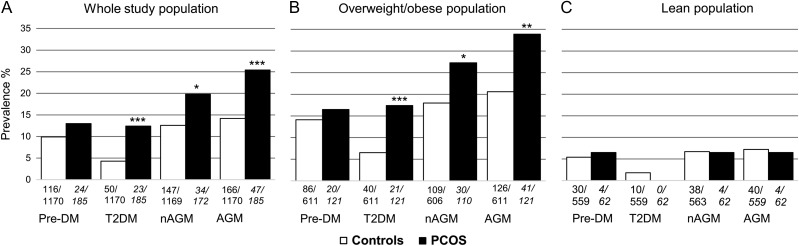
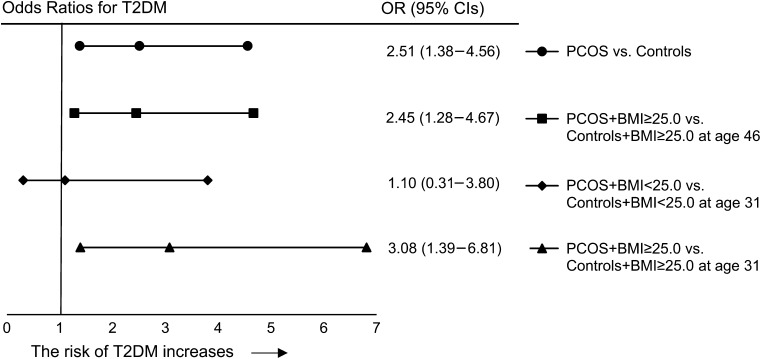
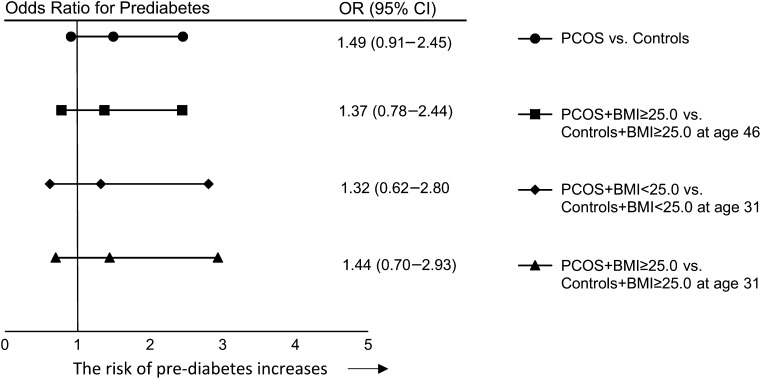
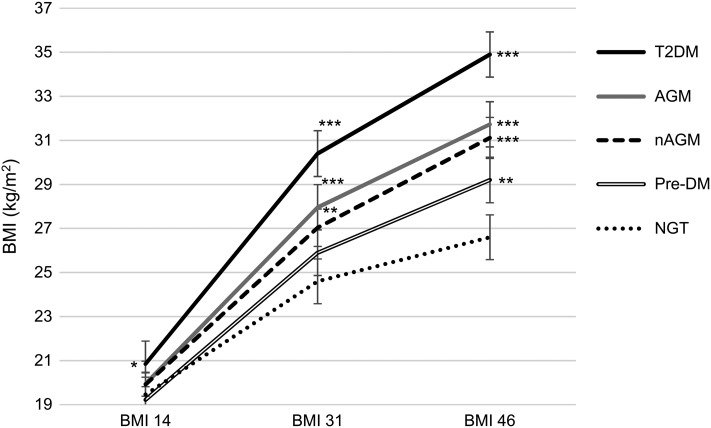
Main results and the role of chance: PCOS per se significantly increased the risk of T2DM in overweight/obese (BMI ≥ 25.0 kg/m2) women with PCOS when compared to overweight/obese controls (odds ratio: 2.45, 95% CI: 1.28-4.67). Normal weight women with PCOS did not present with an increased risk of prediabetes or T2DM. The increase in weight between ages 14, 31 and 46 years was significantly greater in women with PCOS developing T2DM than in women with PCOS and normal glucose tolerance, with the most significant increase occurring in early adulthood (between 14 and 31 years: median with [25%; 75% quartiles]: 27.25 kg [20.43; 34.78] versus 13.80 kg [8.55; 20.20], P < 0.001).
Limitations, reasons for caution: The diagnosis of PCOS was based on self-reporting, and the questionnaire at 46 years did not distinguish between polycystic ovaries only in ultrasonography and the syndrome. Ovarian ultrasonography was not available to aid the diagnosis of PCOS.
Wider implications of the findings: These results emphasize weight management already during adolescence and early adulthood to prevent the development of T2DM in women with PCOS, as the period between 14 and 31 years seems to be a crucial time-window during which the women with PCOS who are destined to develop T2DM by 46 years of age experience a dramatic weight gain. Furthermore, our results support the view that, particularly in times of limited sources of healthcare systems, OGTT screening should be targeted to overweight/obese women with PCOS rather than to all women with PCOS.
Study funding/competing interests: Finnish Medical Foundation; North Ostrobothnia Regional Fund; Academy of Finland (project grants 104781, 120315, 129269, 1114194, 24300796, Center of Excellence in Complex Disease Genetics and SALVE); Sigrid Juselius Foundation; Biocenter Oulu; University Hospital Oulu and University of Oulu (75617); Medical Research Center Oulu; National Institute for Health Research (UK); National Heart, Lung, and Blood Institute (grant 5R01HL087679-02) through the STAMPEED program (1RL1MH083268-01); National Institute of Health/National Institute of Mental Health (5R01MH63706:02); ENGAGE project and grant agreement HEALTH-F4-2007-201413; EU FP7 EurHEALTHAgeing-277849 European Commission and Medical Research Council, UK (G0500539, G0600705, G1002319, PrevMetSyn/SALVE) and Medical Research Center, Centenary Early Career Award. The authors have no conflicts of interests.
Trial registration number: N/A.
Keywords: BMI; Polycystic ovary syndrome; Type 2 diabetes mellitus; prediabetes; weight gain.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 1998;15:539–553. - PubMed
-
- Anonymous Evidence-based Guidelines for the Assessment and Management of Polycystic Ovary Syndrome. Jean Hailes for Women's Health on behalf of the PCOS Australian Alliance. 2015. Melbourne: Available online at https://jeanhailes.org.au/health-professionals/tools (16 December 2016, date last accessed).
-
- Boudreaux MY, Talbott EO, Kip KE, Brooks MM, Witchel SF. Risk of T2DM and impaired fasting glucose among PCOS subjects: results of an 8-year follow-up. Curr Diab Rep 2006;6:77–83. - PubMed
-
- Celik C, Tasdemir N, Abali R, Bastu E, Yilmaz M. Progression to impaired glucose tolerance or type 2 diabetes mellitus in polycystic ovary syndrome: a controlled follow-up study. Fertil Steril 2014;101:1123–1128. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
