

Systemic therapy of brain metastases: non-small cell lung cancer, breast cancer, and melanoma
- PMID: 28031389
- PMCID: PMC5193029
- DOI: 10.1093/neuonc/now197
Systemic therapy of brain metastases: non-small cell lung cancer, breast cancer, and melanoma
Abstract
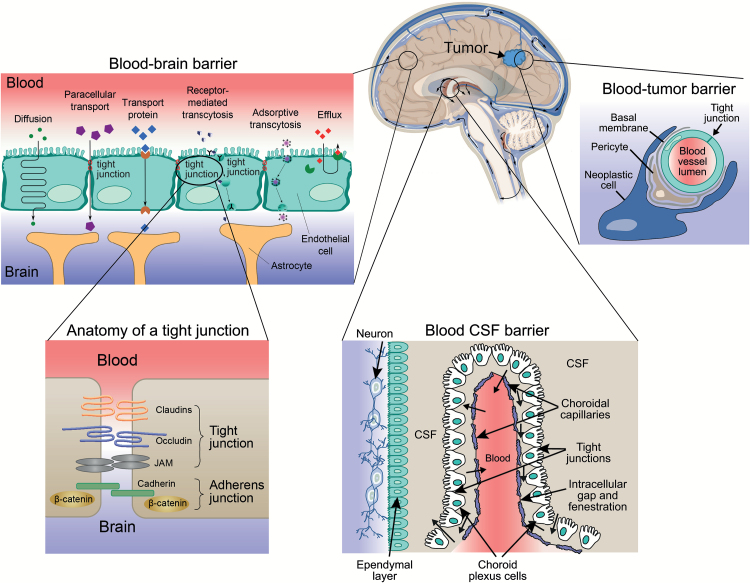
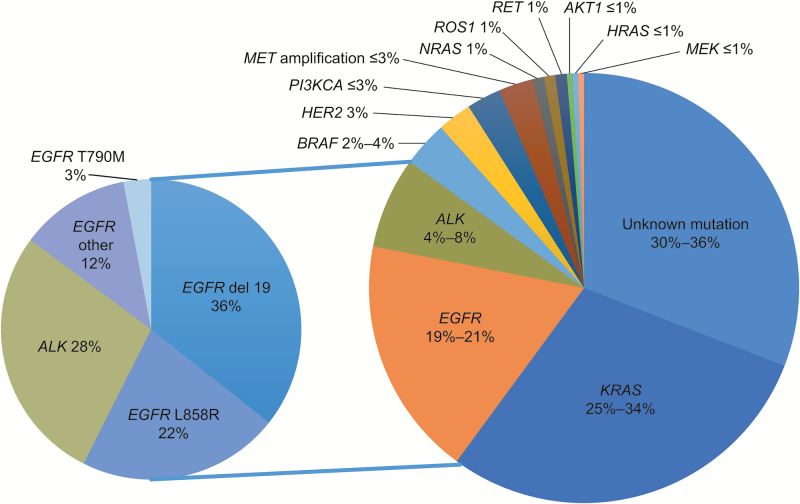
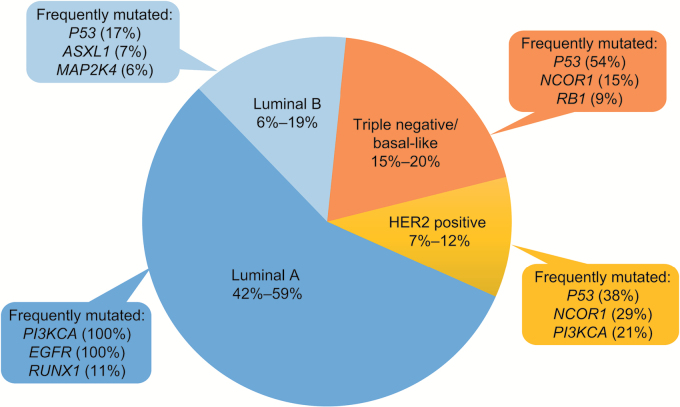
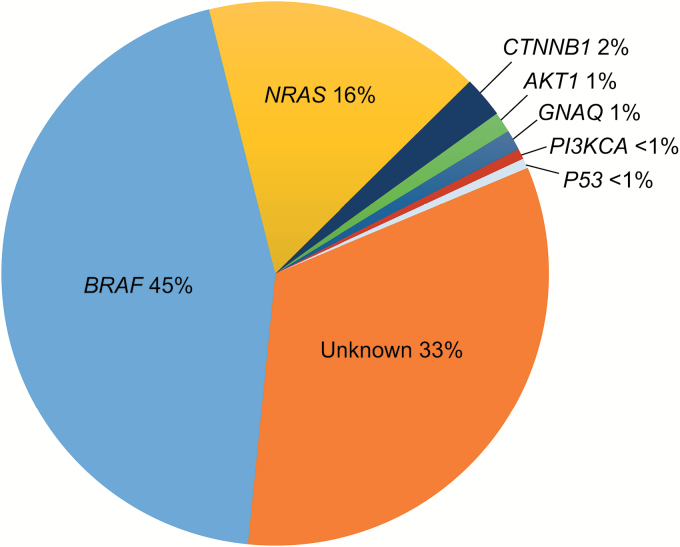
Brain metastases (BM) occur frequently in many cancers, particularly non-small cell lung cancer (NSCLC), breast cancer, and melanoma. The development of BM is associated with poor prognosis and has an adverse impact on survival and quality of life. Commonly used therapies for BM such as surgery or radiotherapy are associated with only modest benefits. However, recent advances in systemic therapy of many cancers have generated considerable interest in exploration of those therapies for treatment of intracranial metastases.This review discusses the epidemiology of BM from the aforementioned primary tumors and the challenges of using systemic therapies for metastatic disease located within the central nervous system. Cumulative data from several retrospective and small prospective studies suggest that molecularly targeted systemic therapies may be an effective option for the treatment of BM from NSCLC, breast cancer, and melanoma, either as monotherapy or in conjunction with other therapies. Larger prospective studies are warranted to further characterize the efficacy and safety profiles of these targeted agents for the treatment of BM.
Keywords: Brain metastases; blood-brain barrier; breast cancer; melanoma; non–small cell lung cancer.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the metropolitan Detroit cancer surveillance system. J Clin Oncol. 2004;22(14):2865–2872. - PubMed
-
- Hall WA, Djalilian HR, Nussbaum ES, Cho KH. Long-term survival with metastatic cancer to the brain. Med Oncol. 2000;17(4):279–286. - PubMed
-
- Schouten LJ, Rutten J, Huveneers HA, Twijnstra A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer. 2002;94(10):2698–2705. - PubMed
-
- Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol. 2005;75(1):5–14. - PubMed
-
- Tabouret E, Chinot O, Metellus P, Tallet A, Viens P, Gonçalves A. Recent trends in epidemiology of brain metastases: an overview. Anticancer Res. 2012;32(11):4655–4662. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
