

Sarcoidosis in the setting of combination ipilimumab and nivolumab immunotherapy: a case report & review of the literature
- PMID: 28031822
- PMCID: PMC5168862
- DOI: 10.1186/s40425-016-0199-9
Sarcoidosis in the setting of combination ipilimumab and nivolumab immunotherapy: a case report & review of the literature
Abstract
Background: We report a case of sarcoidosis in a patient with metastatic melanoma managed with combination ipilimumab/nivolumab. Sarcoid development has been linked with single agent immunotherapy but, to our knowledge, it has not been reported with combination ipilimumab/nivolumab treatment. This case raises unique management challenges for both the melanoma and the immunotherapy-related toxicity.
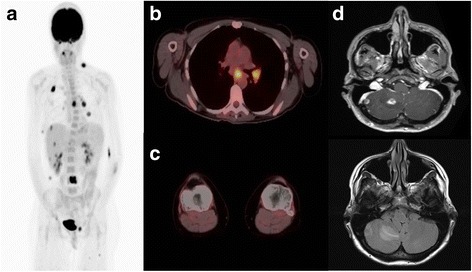
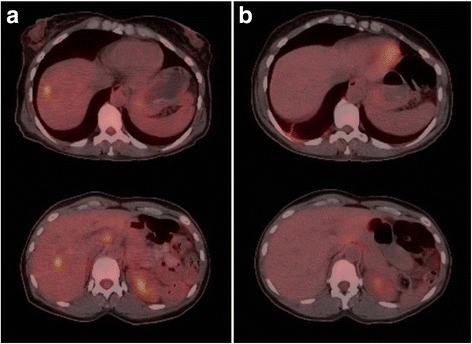
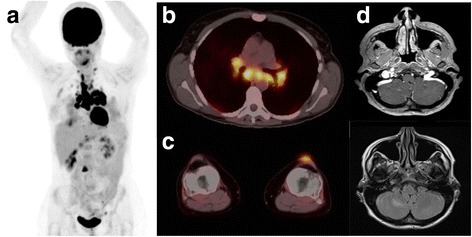
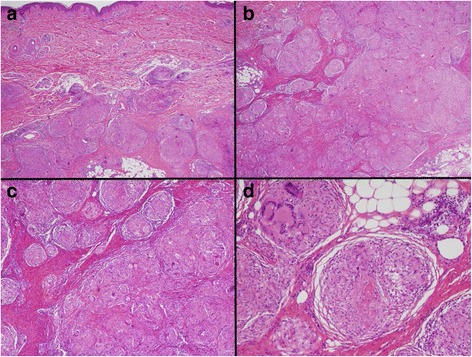
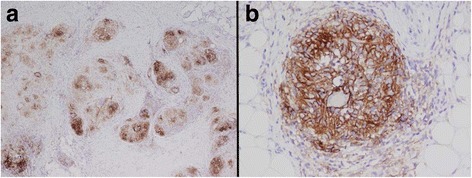
Case presentation: A 46 year old Caucasian female with M1c-metastatic melanoma was managed with ipilimumab/nivolumab combination. Patient experienced response in baseline lesions but developed new clinical and radiographic findings. Biopsy of new lesions at two different sites both demonstrated tumefactive sarcoidosis. Staining of the biopsy tissue for PD-L1 expression demonstrated strong PD-L1 staining of the histiocytes and lymphocytes within the granulomas. Monotherapy nivolumab was continued without progression of sarcoid findings or clinical deterioration.
Conclusions: Tissue biopsy for evaluation of new lesions on immunotherapy is an important step to help guide decision making, as non-melanoma lesions can mimic disease progression.
Keywords: Checkpoint inhibitor; Combination immunotherapy; Immune-related adverse event; Ipilimumab; Metastatic melanoma; Nivolumab; Sarcoidosis.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials