

Relationship between age and erectile dysfunction diagnosis or treatment using real-world observational data in the USA
- PMID: 28032424
- PMCID: PMC5540144
- DOI: 10.1111/ijcp.12908
Relationship between age and erectile dysfunction diagnosis or treatment using real-world observational data in the USA
Abstract
Aims: With self-reporting of erectile dysfunction (ED) in population-based surveys, men with ED may not represent men who are bothered sufficiently to seek an ED diagnosis and treatment. We used real-world observational data to assess: 1) the prevalence of ED diagnosis or treatment by age subgroups; and 2) the relationship of age with ED diagnosis or treatment after controlling for ED-related comorbidities in the USA.
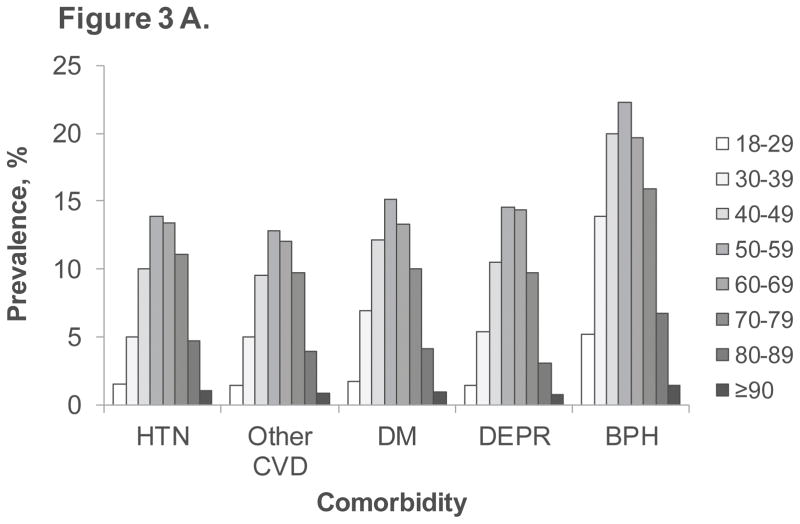
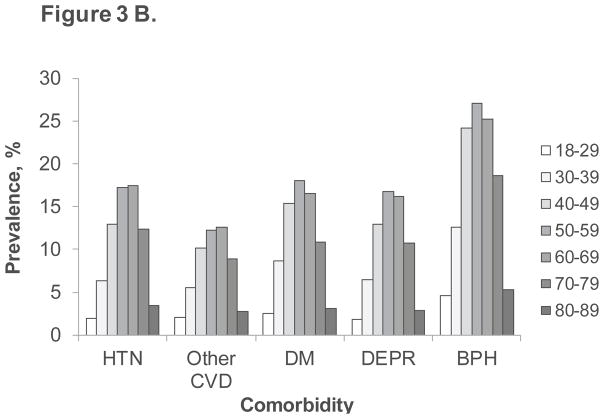
Methods: This cross-sectional study used de-identified claims data (MarketScan® databases; primary analysis). Sensitivity analysis was conducted using electronic health records (Humedica® database). Inclusion criteria were men aged ≥18 years with a 360-day continuous enrollment before the index date. We assessed the prevalence of ED diagnosis or phosphodiesterase type 5 inhibitor (PDE5I) prescription by age and the risk for ED diagnosis or treatment by age after controlling for comorbidities (hypertension, other cardiovascular disease, diabetes mellitus, depression and benign prostatic hyperplasia).
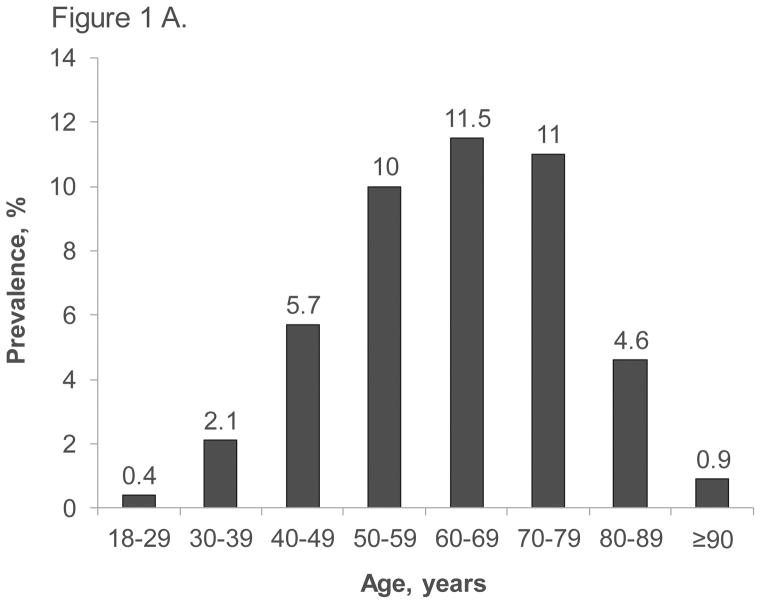
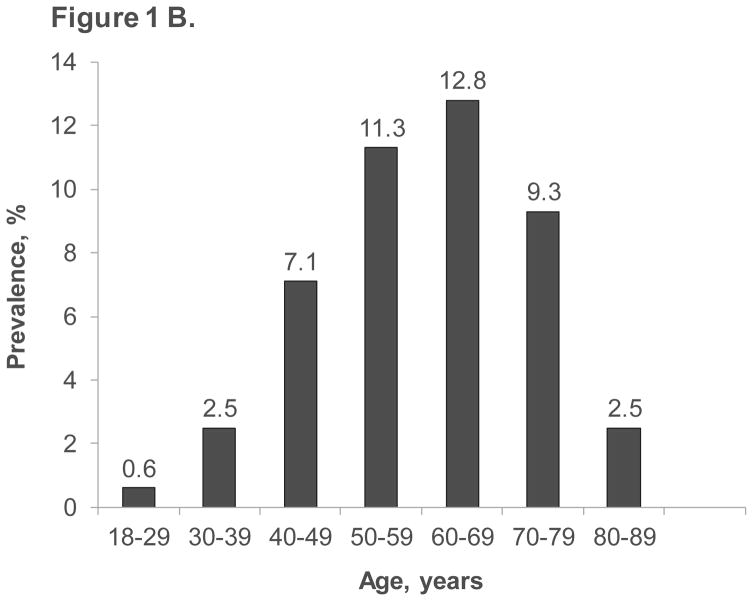
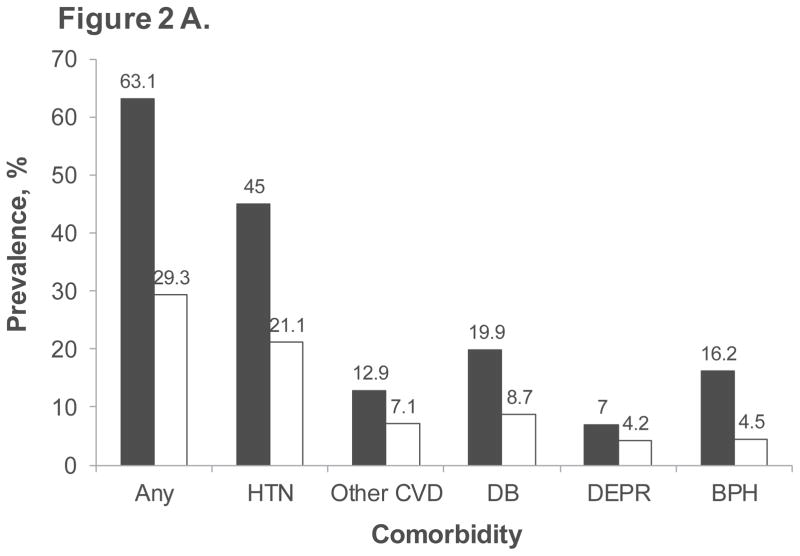
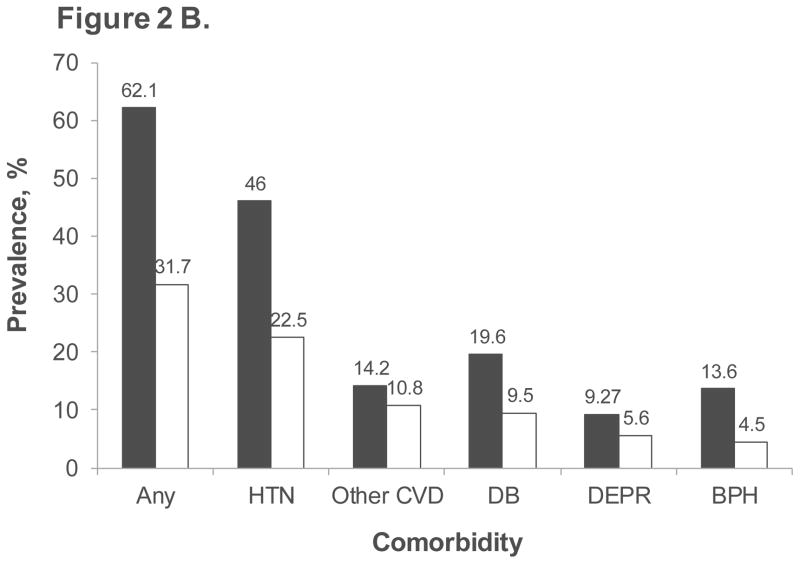
Results: Of 19,833,939 men meeting inclusion criteria in the primary analysis, only 1 108 842 (5.6%) had an ED diagnosis or PDE5I prescription (mean [SD] age: 55.2 [11.2] years). Prevalence of ED diagnosis or treatment increased from age 18-29 years (0.4%) to 60-69 years (11.5%), then decreased in the seventh (11.0%), eighth (4.6%), and ninth (0.9%) decades. Men with ED diagnosis or treatment had a higher prevalence of any comorbidity (63.1% vs 29.3% for men without ED) and of each comorbid condition. In multivariate analyses, age was an independent risk factor for ED diagnosis or treatment. Sensitivity analysis provided consistent results.
Conclusions: In a real-world setting in the USA, the prevalence of ED diagnosis or PDE5I treatment is generally low, increases with age, decreases in very old men, and is associated with increased prevalence of comorbidities. Age is an independent risk factor for ED diagnosis or treatment after controlling for comorbidities.
Keywords: age groups; comorbidity; electronic health records; erectile dysfunction; observational study; phosphodiesterase type 5 inhibitors; real-world claims data.
© 2016 John Wiley & Sons Ltd.
Figures
Comment in
-
Re: Relationship between Age and Erectile Dysfunction Diagnosis or Treatment Using Real-World Observational Data in the USA.J Urol. 2017 Aug;198(2):235-236. doi: 10.1016/j.juro.2017.04.047. Epub 2017 Apr 12. J Urol. 2017. PMID: 29370612 No abstract available.
References
-
- NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA. 1993;270:83–90. - PubMed
-
- Laumann EO, West S, Glasser D, et al. Prevalence and correlates of erectile dysfunction by race and ethnicity among men aged 40 or older in the United States: from the male attitudes regarding sexual health survey. J Sex Med. 2007;4:57–65. - PubMed
-
- Saigal CS, Wessells H, Pace J, et al. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166:207–12. - PubMed
-
- Shabsigh R, Perelman MA, Lockhart DC, et al. Health issues of men: prevalence and correlates of erectile dysfunction. J Urol. 2005;174:662–7. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical