

Validation of Fully Automated VMAT Plan Generation for Library-Based Plan-of-the-Day Cervical Cancer Radiotherapy
- PMID: 28033342
- PMCID: PMC5199117
- DOI: 10.1371/journal.pone.0169202
Validation of Fully Automated VMAT Plan Generation for Library-Based Plan-of-the-Day Cervical Cancer Radiotherapy
Abstract
Purpose: To develop and validate fully automated generation of VMAT plan-libraries for plan-of-the-day adaptive radiotherapy in locally-advanced cervical cancer.
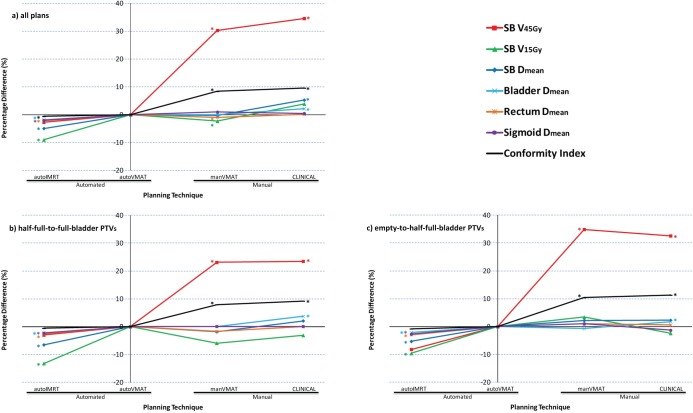
Material and methods: Our framework for fully automated treatment plan generation (Erasmus-iCycle) was adapted to create dual-arc VMAT treatment plan libraries for cervical cancer patients. For each of 34 patients, automatically generated VMAT plans (autoVMAT) were compared to manually generated, clinically delivered 9-beam IMRT plans (CLINICAL), and to dual-arc VMAT plans generated manually by an expert planner (manVMAT). Furthermore, all plans were benchmarked against 20-beam equi-angular IMRT plans (autoIMRT). For all plans, a PTV coverage of 99.5% by at least 95% of the prescribed dose (46 Gy) had the highest planning priority, followed by minimization of V45Gy for small bowel (SB). Other OARs considered were bladder, rectum, and sigmoid.
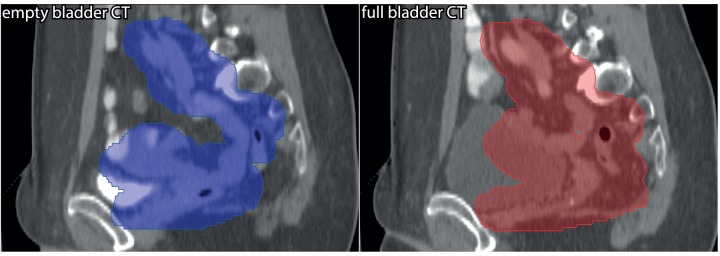
Results: All plans had a highly similar PTV coverage, within the clinical constraints (above). After plan normalizations for exactly equal median PTV doses in corresponding plans, all evaluated OAR parameters in autoVMAT plans were on average lower than in the CLINICAL plans with an average reduction in SB V45Gy of 34.6% (p<0.001). For 41/44 autoVMAT plans, SB V45Gy was lower than for manVMAT (p<0.001, average reduction 30.3%), while SB V15Gy increased by 2.3% (p = 0.011). AutoIMRT reduced SB V45Gy by another 2.7% compared to autoVMAT, while also resulting in a 9.0% reduction in SB V15Gy (p<0.001), but with a prolonged delivery time. Differences between manVMAT and autoVMAT in bladder, rectal and sigmoid doses were ≤ 1%. Improvements in SB dose delivery with autoVMAT instead of manVMAT were higher for empty bladder PTVs compared to full bladder PTVs, due to differences in concavity of the PTVs.
Conclusions: Quality of automatically generated VMAT plans was superior to manually generated plans. Automatic VMAT plan generation for cervical cancer has been implemented in our clinical routine. Due to the achieved workload reduction, extension of plan libraries has become feasible.
Conflict of interest statement
This study is partially funded by Elekta (www.elekta.com), which develops tools and treatment planning systems for radiation therapy, and the Dutch Cancer Society (Grant EMCR 2012-5396).
Figures
References
-
- Chen MF, Tseng CJ, Tseng CC, Kuo YC, Yu CY, Chen WC. Clinical outcome in posthysterectomy cervical cancer patients treated with concurrent Cisplatin and intensity-modulated pelvic radiotherapy: comparison with conventional radiotherapy. Int J Radiat Oncol Biol Phys 2007;67:1438–44. 10.1016/j.ijrobp.2006.11.005 - DOI - PubMed
-
- Mundt AJ, Lujan AE, Rotmensch J, Waggoner SE, Yamada SD, Fleming G, et al. Intensity-modulated whole pelvic radiotherapy in women with gynecologic malignancies. Int J Radiat Oncol Biol Phys 2002;52:1330–7. - PubMed
-
- van de Bunt L, van der Heide UA, Ketelaars M, de Kort GA, Jurgenliemk-Schulz IM. Conventional, conformal, and intensity-modulated radiation therapy treatment planning of external beam radiotherapy for cervical cancer: The impact of tumor regression. Int J Radiat Oncol Biol Phys 2006;64:189–96. 10.1016/j.ijrobp.2005.04.025 - DOI - PubMed
-
- Ahmad R, Hoogeman MS, Bondar ML, Dhawtal V, Quint S, De Pree l, et al. Increasing treatment accuracy for cervical cancer patients using correlations between bladder-filling change and cervix-uterus displacements: proof of principle. Radiother Oncol 2011;98:340–6. 10.1016/j.radonc.2010.11.010 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
