

The influence of interpregnancy interval on infant mortality
- PMID: 28034653
- PMCID: PMC5356481
- DOI: 10.1016/j.ajog.2016.12.018
The influence of interpregnancy interval on infant mortality
Abstract
Background: In Ohio, the infant mortality rate is above the national average and the black infant mortality rate is more than twice the white infant mortality rate. Having a short interpregnancy interval has been shown to correlate with preterm birth and low birthweight, but the effect of short interpregnancy interval on infant mortality is less well established.
Objective: We sought to quantify the population impact of interpregnancy interval on the risk of infant mortality.
Study design: This was a statewide population-based retrospective cohort study of all births (n = 1,131,070) and infant mortalities (n = 8152) using linked Ohio birth and infant death records from January 2007 through September 2014. For this study we analyzed 5 interpregnancy interval categories: 0-<6, 6-<12, 12-<24, 24-<60, and ≥60 months. The primary outcome for this study was infant mortality. During the study period, 3701 infant mortalities were linked to a live birth certificate with an interpregnancy interval available. We calculated the frequency and relative risk of infant mortality for each interval compared to a referent interval of 12-<24 months. Stratified analyses by maternal race were also performed. Adjusted risks were estimated after accounting for statistically significant and biologically plausible confounding variables. Adjusted relative risk was utilized to calculate the attributable risk percent of short interpregnancy intervals on infant mortality.
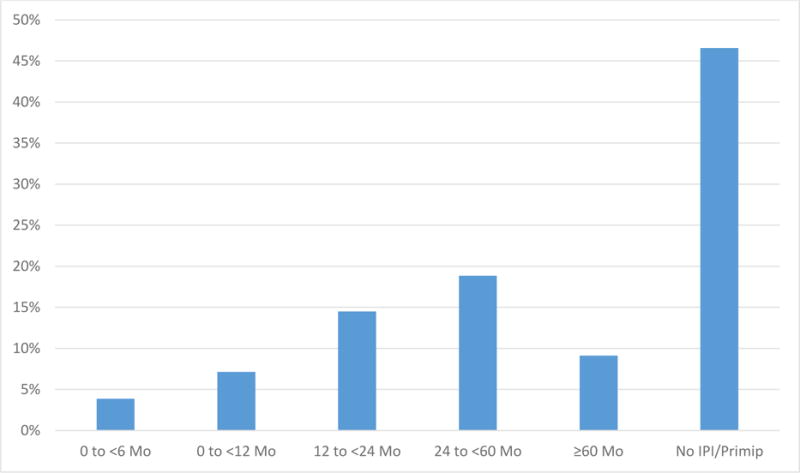
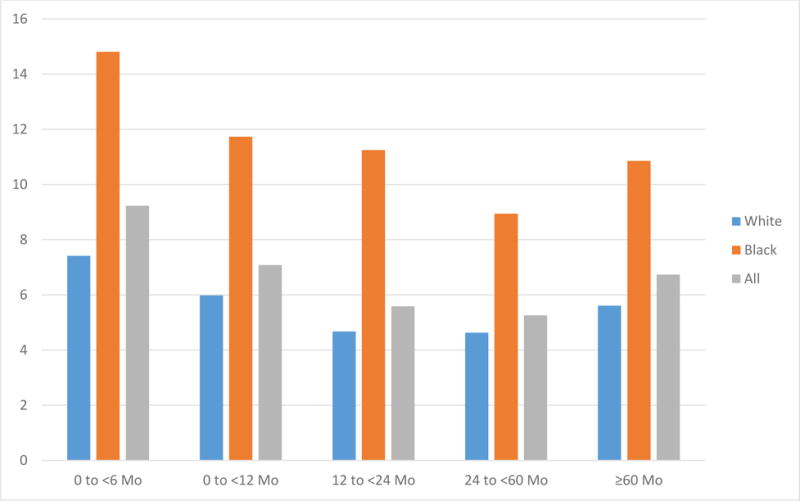
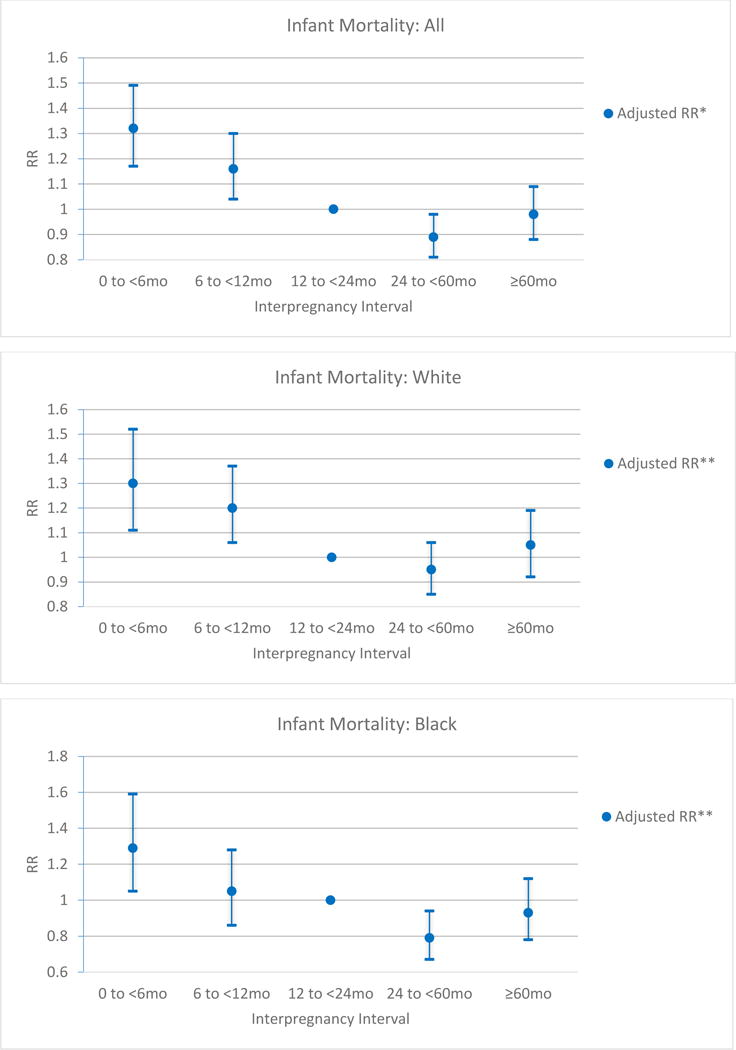
Results: Short interpregnancy intervals were common in Ohio during the study period. Of all multiparous births, 20.5% followed an interval of <12 months. The overall infant mortality rate during this time was 7.2 per 1000 live births (6.0 for white mothers and 13.1 for black mothers). Infant mortalities occurred more frequently for births following short intervals of 0-<6 months (9.2 per 1000) and 6-<12 months (7.1 per 1000) compared to 12-<24 months (5.6 per 1000) (P < .001 and <.001). The highest risk for infant mortality followed interpregnancy intervals of 0-<6 months (adjusted relative risk, 1.32; 95% confidence interval, 1.17-1.49) followed by interpregnancy intervals of 6-<12 months (adjusted relative risk, 1.16; 95% confidence interval, 1.04-1.30). Analysis stratified by maternal race revealed similar findings. Attributable risk calculation showed that 24.2% of infant mortalities following intervals of 0-<6 months and 14.1% with intervals of 6-<12 months are attributable to the short interpregnancy interval. By avoiding short interpregnancy intervals of ≤12 months we estimate that in the state of Ohio 31 infant mortalities (20 white and 8 black) per year could have been prevented and the infant mortality rate could have been reduced from 7.2-7.0 during this time frame.
Conclusion: An interpregnancy interval of 12-60 months (1-5 years) between birth and conception of next pregnancy is associated with lowest risk of infant mortality. Public health initiatives and provider counseling to optimize birth spacing has the potential to significantly reduce infant mortality for both white and black mothers.
Keywords: infant mortality; interpregnancy interval.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure Statement: The authors report no conflicts of interest.
Figures

References
-
- Atreya MR, Muglia LJ, Greenberg JM, DeFranco EA. Racial Differences in the Influence of Interpregnancy Interval on Fetal Growth. Matern Child Health J. 2016 Jul 30; [Epub ahead of print] - PubMed
-
- Brody DJ, Bracken MB. Short interpregnancy interval: a risk factor for low birthweight. Am J Perinatol. 1987 Jan;4(1):50–4. - PubMed
-
- Centers for Disease Control and Prevention [Internet] Atlanta [updated 2016 Jan 12; cited 2016 July 28] Infant Mortality. Available from: http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/InfantMortali....
-
- Chen I, Jhangri GS, Chandra S. Relationship between interpregnancy interval and congenital anomalies. Am J Obstet Gynecol. 2014 Jun;210(6):564.e1–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
