

Polyclonal Secondary FGFR2 Mutations Drive Acquired Resistance to FGFR Inhibition in Patients with FGFR2 Fusion-Positive Cholangiocarcinoma
- PMID: 28034880
- PMCID: PMC5433349
- DOI: 10.1158/2159-8290.CD-16-1000
Polyclonal Secondary FGFR2 Mutations Drive Acquired Resistance to FGFR Inhibition in Patients with FGFR2 Fusion-Positive Cholangiocarcinoma
Abstract
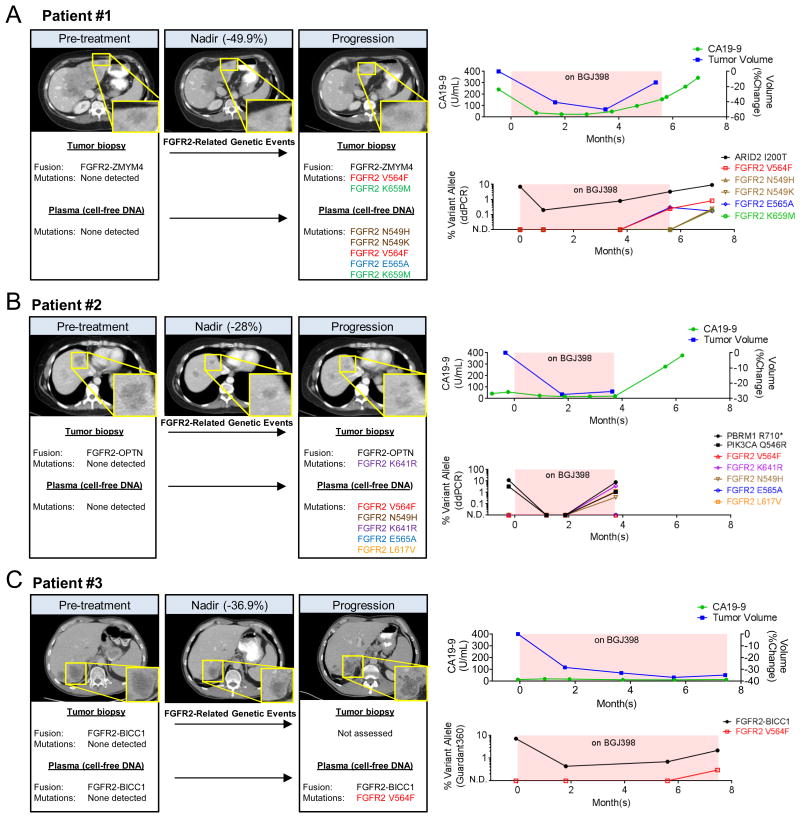
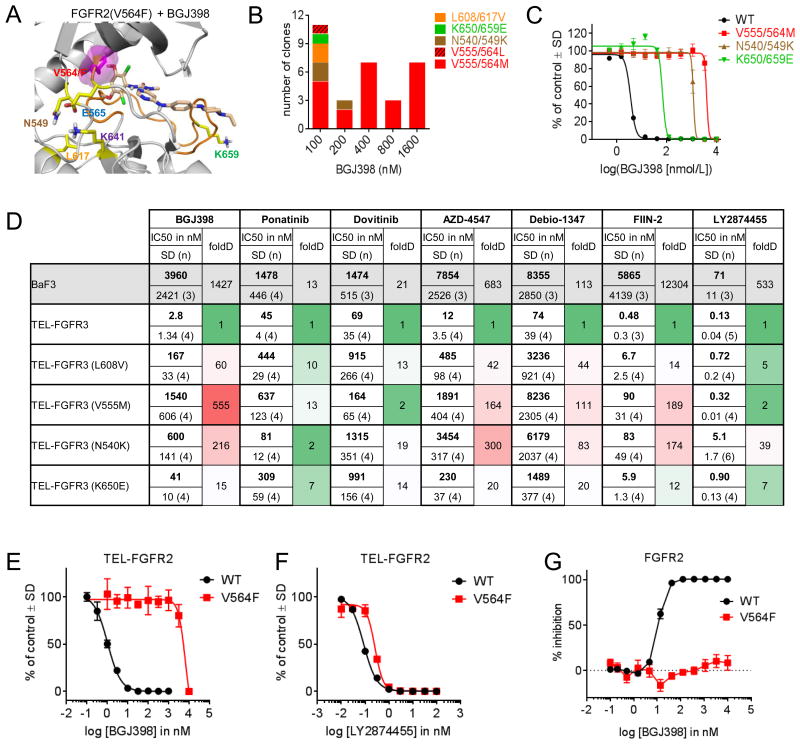
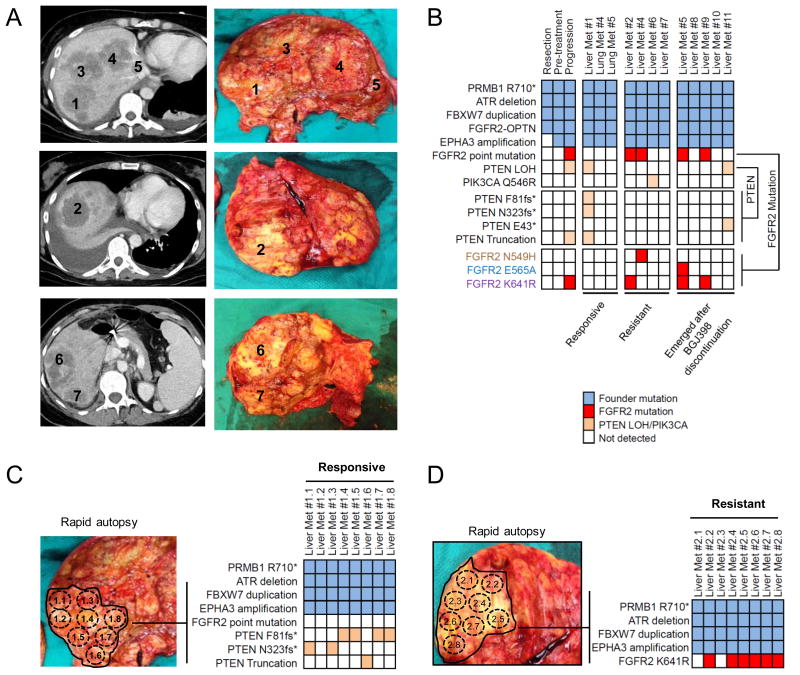
Genetic alterations in the fibroblast growth factor receptor (FGFR) pathway are promising therapeutic targets in many cancers, including intrahepatic cholangiocarcinoma (ICC). The FGFR inhibitor BGJ398 displayed encouraging efficacy in patients with FGFR2 fusion-positive ICC in a phase II trial, but the durability of response was limited in some patients. Here, we report the molecular basis for acquired resistance to BGJ398 in three patients via integrative genomic characterization of cell-free circulating tumor DNA (cfDNA), primary tumors, and metastases. Serial analysis of cfDNA demonstrated multiple recurrent point mutations in the FGFR2 kinase domain at progression. Accordingly, biopsy of post-progression lesions and rapid autopsy revealed marked inter- and intralesional heterogeneity, with different FGFR2 mutations in individual resistant clones. Molecular modeling and in vitro studies indicated that each mutation led to BGJ398 resistance and was surmountable by structurally distinct FGFR inhibitors. Thus, polyclonal secondary FGFR2 mutations represent an important clinical resistance mechanism that may guide the development of future therapeutic strategies.Significance: We report the first genetic mechanisms of clinical acquired resistance to FGFR inhibition in patients with FGFR2 fusion-positive ICC. Our findings can inform future strategies for detecting resistance mechanisms and inducing more durable remissions in ICC and in the wide variety of cancers where the FGFR pathway is being explored as a therapeutic target. Cancer Discov; 7(3); 252-63. ©2016 AACR.See related commentary by Smyth et al., p. 248This article is highlighted in the In This Issue feature, p. 235.
©2016 American Association for Cancer Research.
Conflict of interest statement
Figures
Comment in
-
Gatekeeper Mutations and Intratumoral Heterogeneity in FGFR2-Translocated Cholangiocarcinoma.Cancer Discov. 2017 Mar;7(3):248-249. doi: 10.1158/2159-8290.CD-17-0057. Cancer Discov. 2017. PMID: 28264865
References
-
- Turner N, Grose R. Fibroblast growth factor signalling: from development to cancer. Nat Rev Cancer. 2010;10:116–29. - PubMed
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Seminars in liver disease. 2004;24:115–25. - PubMed
-
- Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362:1273–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
