

Impact of Intravenous Immunoglobulin on Survival in Necrotizing Fasciitis With Vasopressor-Dependent Shock: A Propensity Score-Matched Analysis From 130 US Hospitals
- PMID: 28034881
- PMCID: PMC5850528
- DOI: 10.1093/cid/ciw871
Impact of Intravenous Immunoglobulin on Survival in Necrotizing Fasciitis With Vasopressor-Dependent Shock: A Propensity Score-Matched Analysis From 130 US Hospitals
Abstract
Background: Shock frequently complicates necrotizing fasciitis (NF) caused by group A Streptococcus (GAS) or Staphylococcus aureus. Intravenous immunoglobulin (IVIG) is sometimes administered for presumptive toxic shock syndrome (TSS), but its frequency of use and efficacy are unclear.
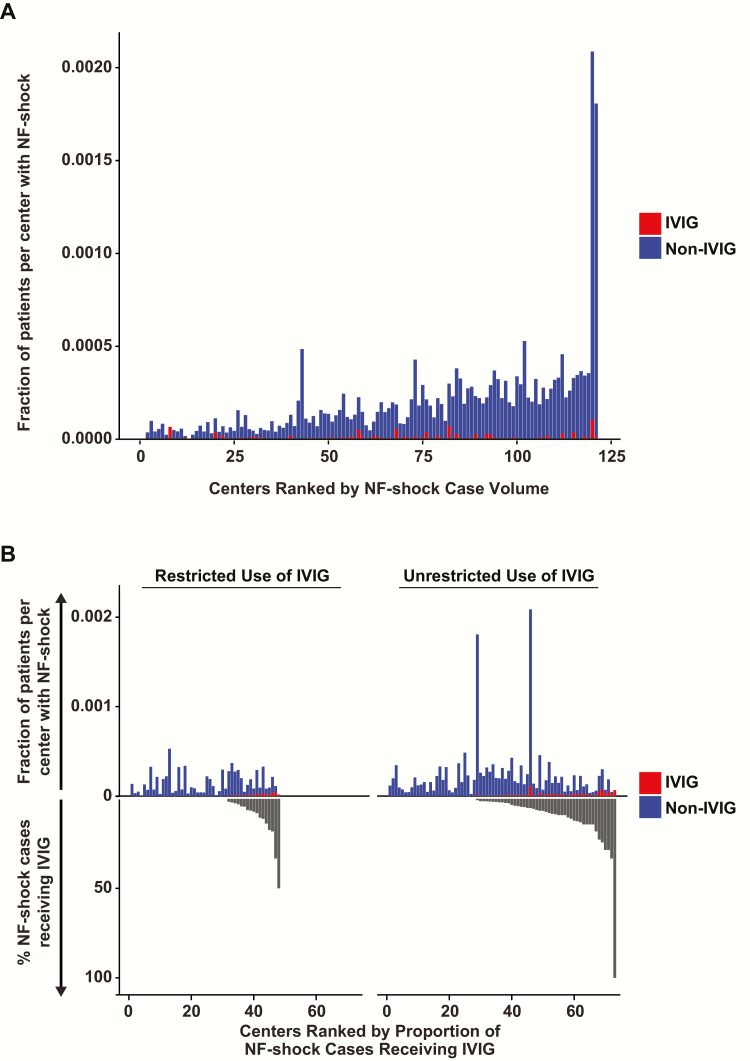
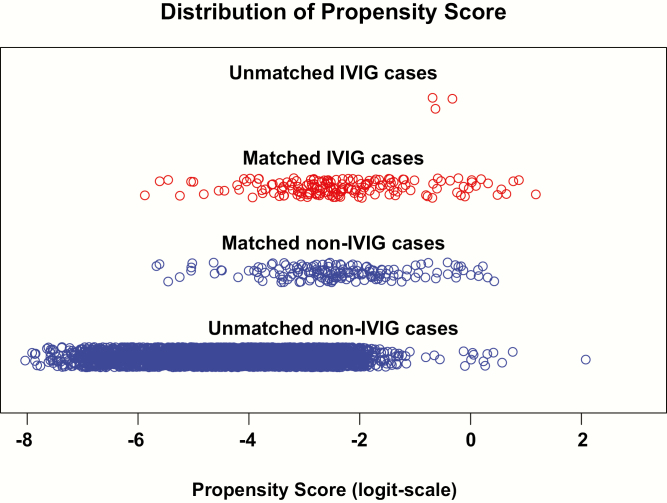
Methods: Adult patients with NF and vasopressor-dependent shock undergoing surgical debridement from 2010 to 2014 were identified at 130 US hospitals. IVIG cases were propensity-matched and risk-adjusted. The primary outcome was in-hospital mortality and the secondary outcome was median length of stay (LOS).
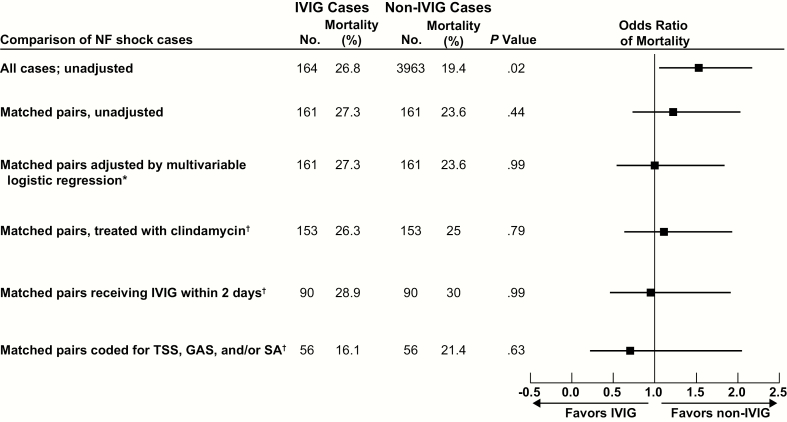
Results: Of 4127 cases of debrided NF with shock at 121 centers, only 164 patients (4%) at 61 centers received IVIG. IVIG subjects were younger with lower comorbidity indices, but higher illness severity. Clindamycin and vasopressor intensity were higher among IVIG cases, as was coding for TSS and GAS. In-hospital mortality did not differ between matched IVIG and non-IVIG groups (crude mortality, 27.3% vs 23.6%; adjusted odds ratio, 1.00 [95% confidence interval, .55-1.83]; P = .99). Early IVIG (≤2 days) did not alter this effect (P = .99). Among patients coded for TSS, GAS, and/or S. aureus, IVIG use was still unusual (59/868 [6.8%]) and lacked benefit (P = .63). Median LOS was similar between IVIG and non-IVIG groups (26 [13-49] vs 26 [11-43]; P = .84). Positive predictive values for identifying true NF and debridement among IVIG cases using our algorithms were 97% and 89%, respectively, based on records review at 4 hospitals.
Conclusions: Adjunctive IVIG was administered infrequently in NF with shock and had no apparent impact on mortality or hospital LOS beyond that achieved with debridement and antibiotics.
Keywords: intravenous immunoglobulin; necrotizing fasciitis.; toxic shock.
Published by Oxford University Press for the Infectious Diseases Society of America 2016. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures

References
-
- Miller LG, Perdreau-Remington F, Rieg G, et al. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med 2005; 352:1445–53. - PubMed
-
- Murray RJ. Recognition and management of Staphylococcus aureus toxin-mediated disease. Intern Med J 2005; 35:S106–19. - PubMed
-
- Lappin E, Ferguson AJ. Gram-positive toxic shock syndromes. Lancet Infect Dis 2009; 9:281–90. - PubMed
-
- McCormick JK, Yarwood JM, Schlievert PM. Toxic shock syndrome and bacterial superantigens: an update. Annu Rev Microbiol 2001; 55:77–104. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
