

An Evidence-Based Algorithm for Early Prognosis of Severe Dengue in the Outpatient Setting
- PMID: 28034883
- PMCID: PMC5850639
- DOI: 10.1093/cid/ciw863
An Evidence-Based Algorithm for Early Prognosis of Severe Dengue in the Outpatient Setting
Abstract
Background: Early prediction of severe dengue could significantly assist patient triage and case management.
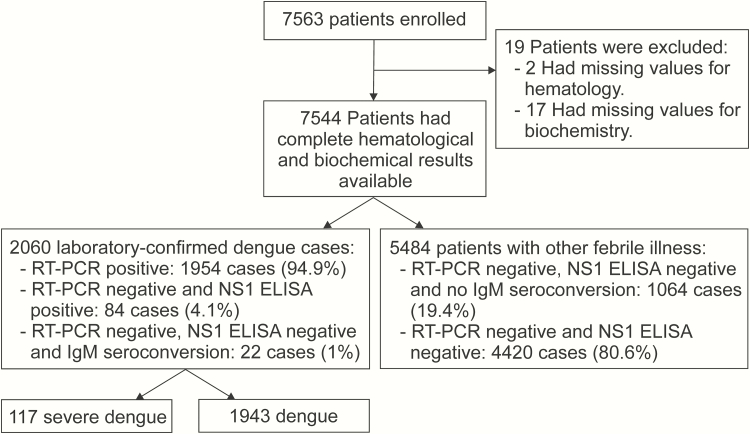
Methods: We prospectively investigated 7563 children with ≤3 days of fever recruited in the outpatient departments of 6 hospitals in southern Vietnam between 2010 and 2013. The primary endpoint of interest was severe dengue (2009 World Health Organization Guidelines), and predefined risk variables were collected at the time of enrollment to enable prognostic model development.
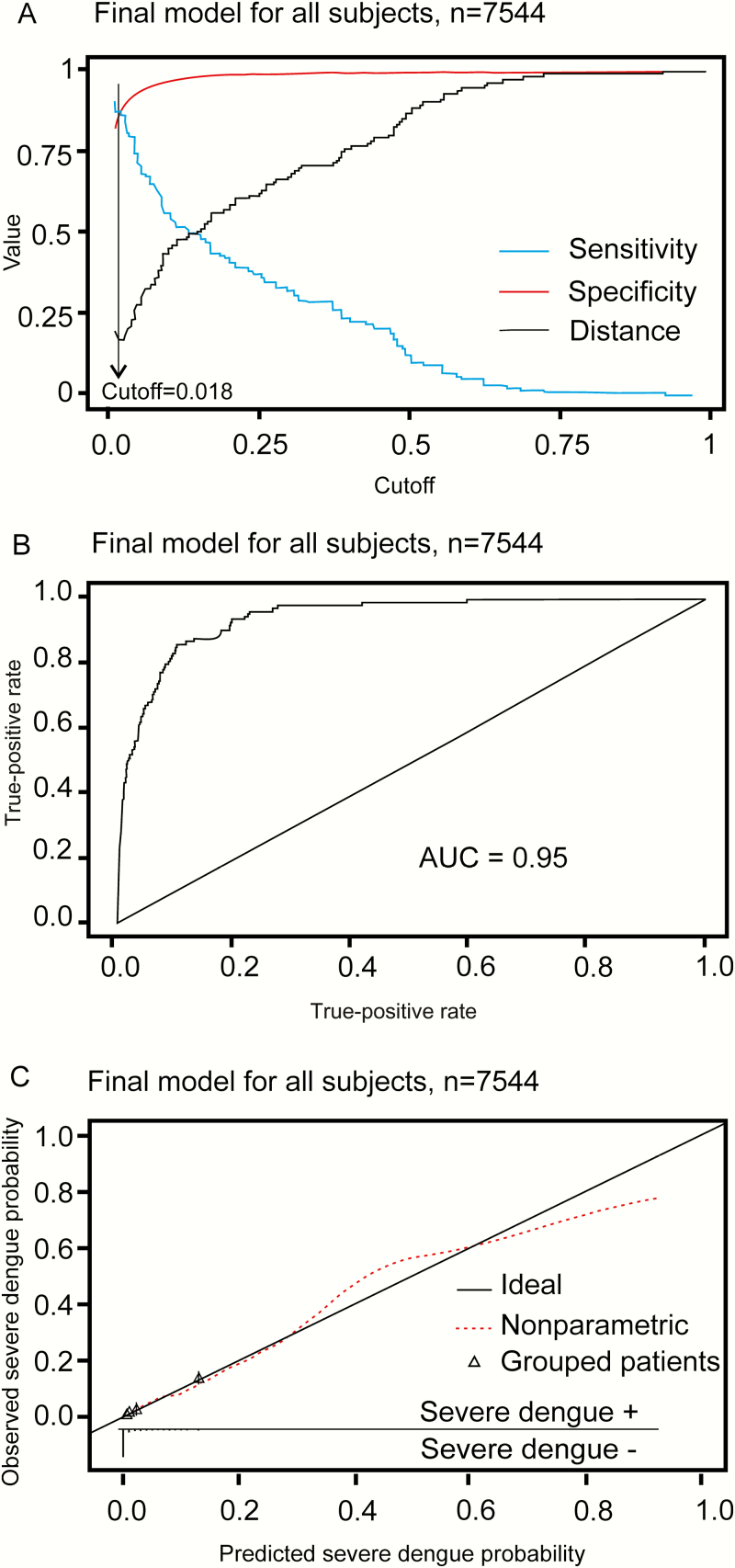
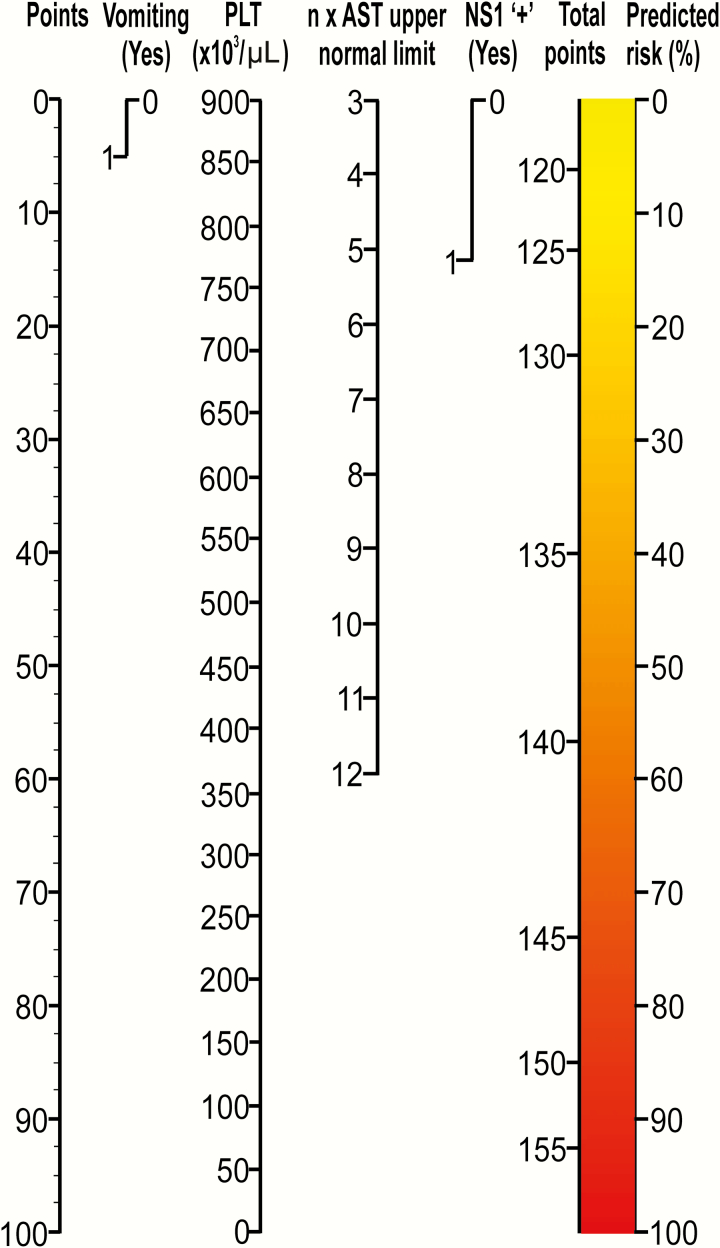
Results: The analysis population comprised 7544 patients, of whom 2060 (27.3%) had laboratory-confirmed dengue; nested among these were 117 (1.5%) severe cases. In the multivariate logistic model, a history of vomiting, lower platelet count, elevated aspartate aminotransferase (AST) level, positivity in the nonstructural protein 1 (NS1) rapid test, and viremia magnitude were all independently associated with severe dengue. The final prognostic model (Early Severe Dengue Identifier [ESDI]) included history of vomiting, platelet count, AST level. and NS1 rapid test status.
Conclusions: The ESDI had acceptable performance features (area under the curve = 0.95, sensitivity 87% (95% confidence interval [CI], 80%-92%), specificity 88% (95% CI, 87%-89%), positive predictive value 10% (95% CI, 9%-12%), and negative predictive value of 99% (95% CI, 98%-100%) in the population of all 7563 enrolled children. A score chart, for routine clinical use, was derived from the prognostic model and could improve triage and management of children presenting with fever in dengue-endemic areas.
Keywords: dengue; diagnosis; tropical infectious diseases..
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Prognosticating Dengue.Clin Infect Dis. 2017 Mar 1;64(5):664-665. doi: 10.1093/cid/ciw867. Clin Infect Dis. 2017. PMID: 28034884 No abstract available.
References
-
- World Health Organization. Dengue: guideline for diagnosis, treatment, prevention and control. Geneva, Switzerland: WHO, 2009. - PubMed
-
- L’Azou M, Moureau A, Sarti E, et al. ; CYD14 Primary Study Group; CYD15 Primary Study Group Symptomatic dengue in children in 10 Asian and Latin American countries. N Engl J Med 2016; 374:1155–66. - PubMed
-
- Martinez-Torres E, Polanco-Anaya AC, Pleites-Sandoval EB. Why and how children with dengue die? Rev Cubana Med Trop 2008; 60:40–7.
-
- Ranjit S, Kissoon N. Dengue hemorrhagic fever and shock syndromes. Pediatr Crit Care Med 2011; 12:90–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
