

Serum B-cell maturation antigen: a novel biomarker to predict outcomes for multiple myeloma patients
- PMID: 28034989
- PMCID: PMC5395119
- DOI: 10.3324/haematol.2016.150896
Serum B-cell maturation antigen: a novel biomarker to predict outcomes for multiple myeloma patients
Abstract
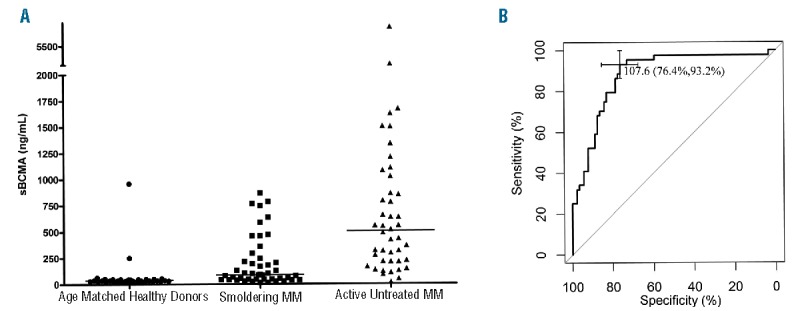
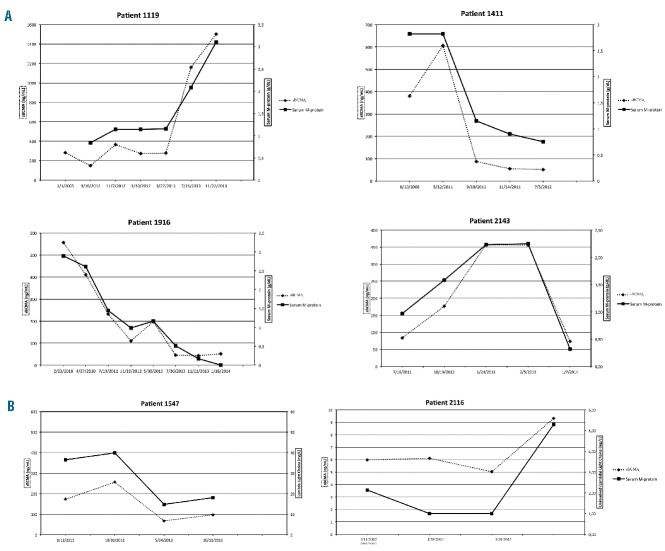
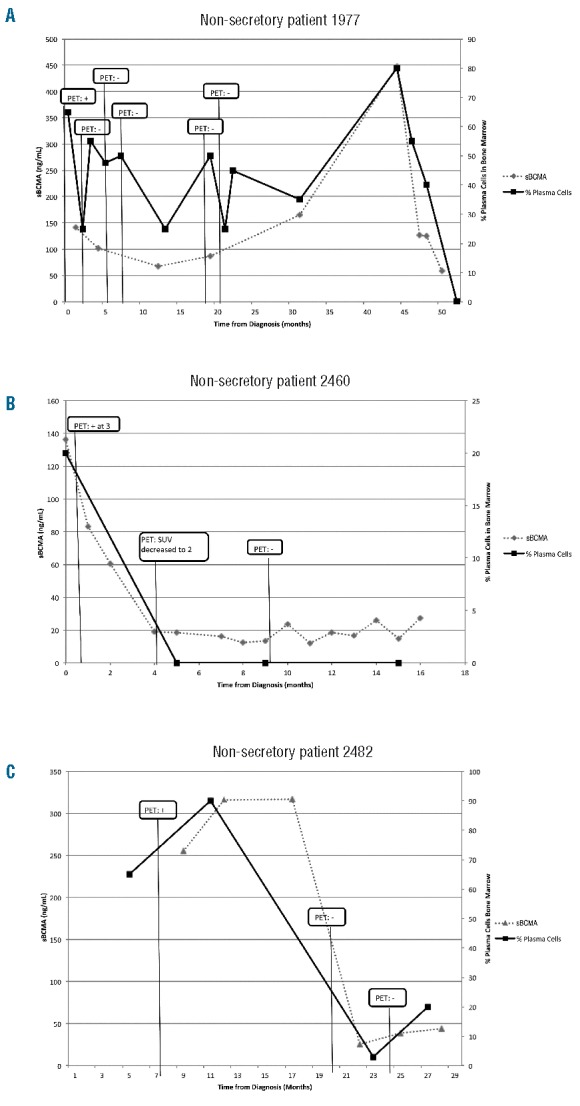
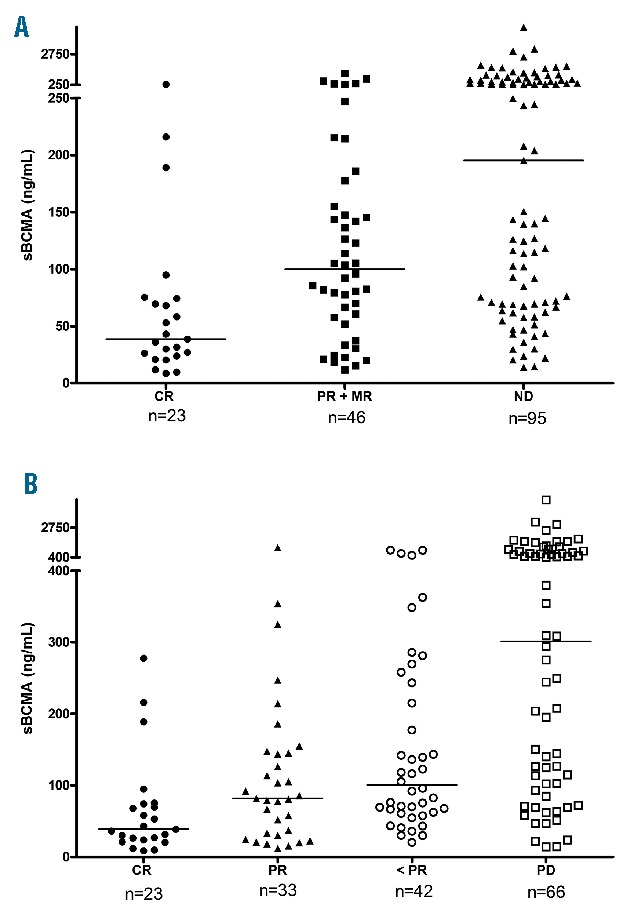
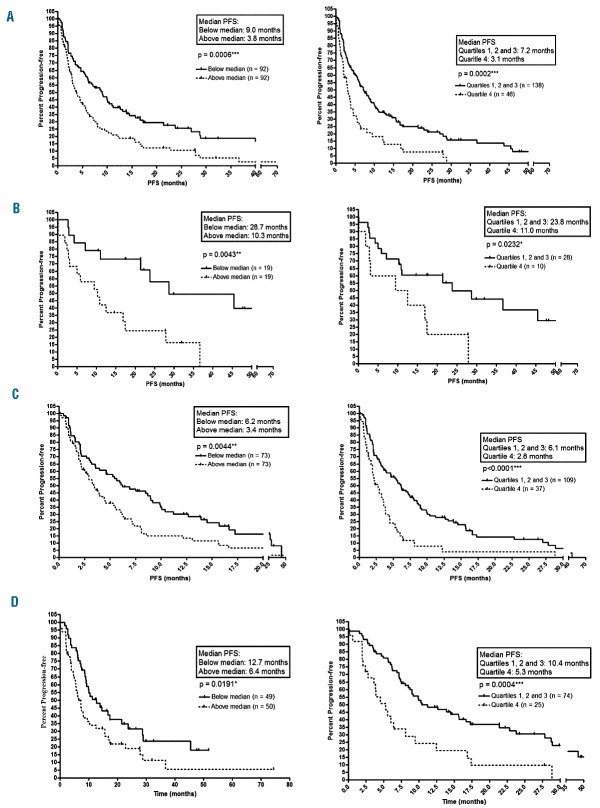
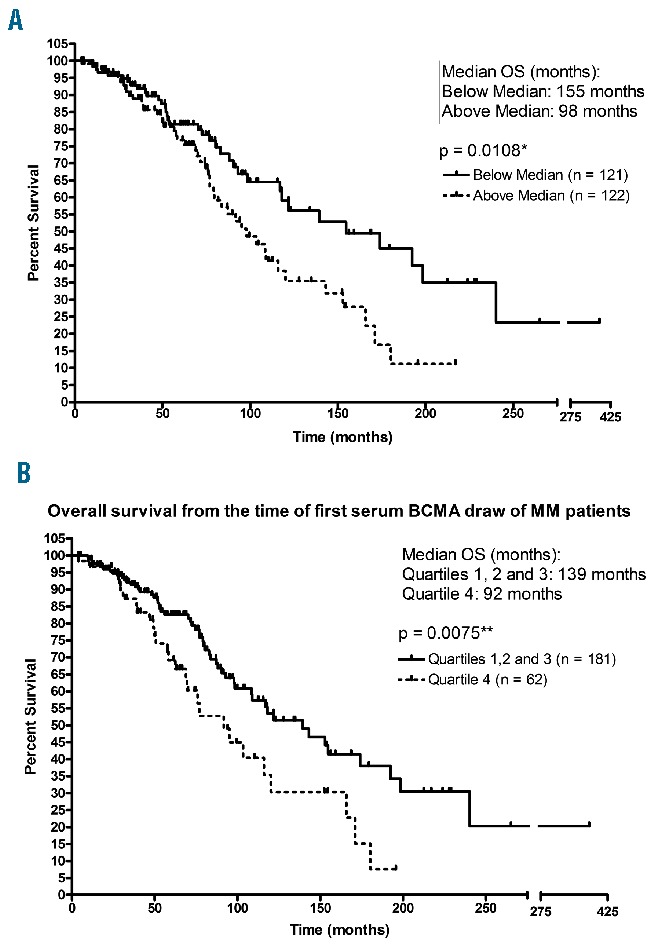
B-cell maturation antigen is expressed on plasma cells. In this study, we have identified serum B-cell maturation antigen as a novel biomarker that can monitor and predict outcomes for multiple myeloma patients. Compared to healthy donors, patients with multiple myeloma showed elevated serum B-cell maturation antigen levels (P<0.0001). Serum B-cell maturation antigen levels correlated with the proportion of plasma cells in bone marrow biopsies (Spearman's rho = 0.710; P<0.001), clinical status (complete response vs partial response, P=0.0374; complete response vs progressive disease, P<0.0001), and tracked with changes in M-protein levels. Among patients with non-secretory disease, serum B-cell maturation antigen levels correlated with bone marrow plasma cell levels and findings from positron emission tomography scans. Kaplan-Meier analysis demonstrated that serum B-cell maturation antigen levels above the median levels were predictive of a shorter progression-free survival (P=0.0006) and overall survival (P=0.0108) among multiple myeloma patients (n=243). Specifically, patients with serum B-cell maturation antigen levels above the median level at the time of starting front-line (P=0.0043) or a new salvage therapy (P=0.0044) were found to have shorter progression-free survival. Importantly, serum B-cell maturation antigen levels did not show any dependence on renal function and maintained independent significance when tested against other known prognostic markers for multiple myeloma such as age, serum β2 microglobulin, hemoglobin, and bone disease. These data identify serum B-cell maturation antigen as a new biomarker to manage multiple myeloma patients.
Copyright© Ferrata Storti Foundation.
Figures

References
-
- Smith ML, Newland AC. Treatment of myeloma. QJM. 1999;92(1):11–16. - PubMed
-
- Morgan GJ. Advances in the biology and treatment of myeloma. Br J Haematol. 1999;105(Suppl 1):4–6. - PubMed
-
- Kastrinakis NG, Gorgoulis VG, Foukas PG, et al. Molecular aspects of multiple myeloma. Ann Oncol. 2000;11(10):1217–1228. - PubMed
-
- van de Donk NW, Moreau P, Plesner T, et al. Clinical efficacy and management of monoclonal antibodies targeting CD38 and SLAMF7 in multiple myeloma. Blood. 2016;127(6):681–695. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
