

Motor Lateralization Provides a Foundation for Predicting and Treating Non-paretic Arm Motor Deficits in Stroke
- PMID: 28035570
- PMCID: PMC5364330
- DOI: 10.1007/978-3-319-47313-0_14
Motor Lateralization Provides a Foundation for Predicting and Treating Non-paretic Arm Motor Deficits in Stroke
Abstract
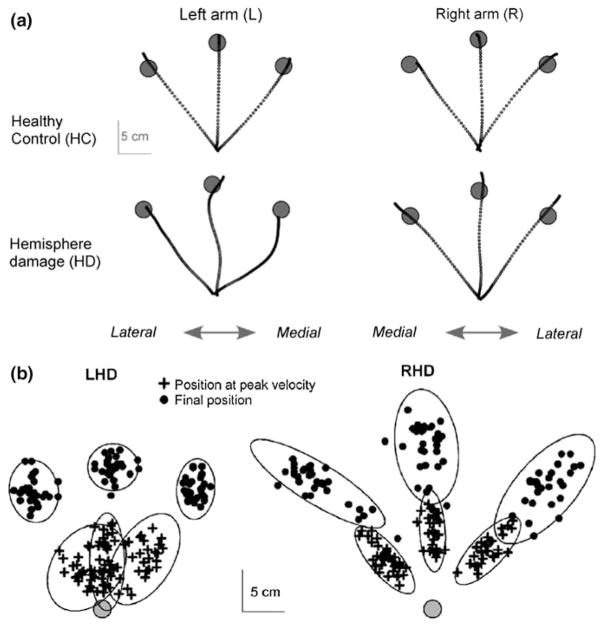
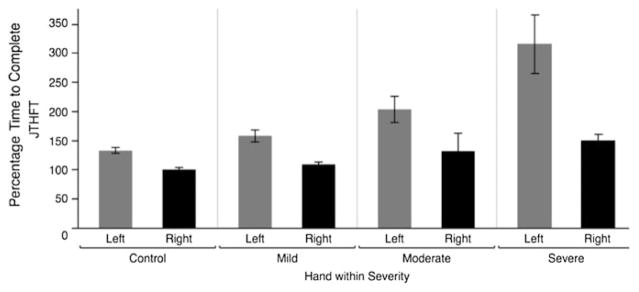
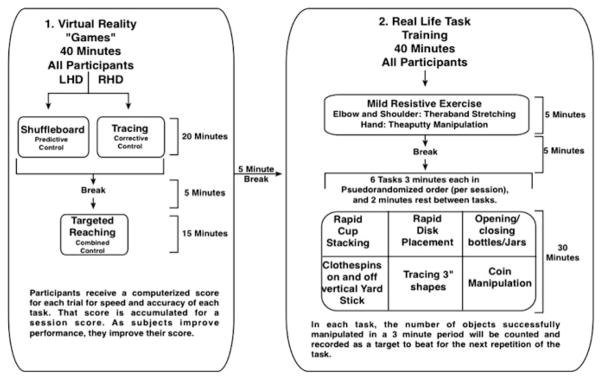
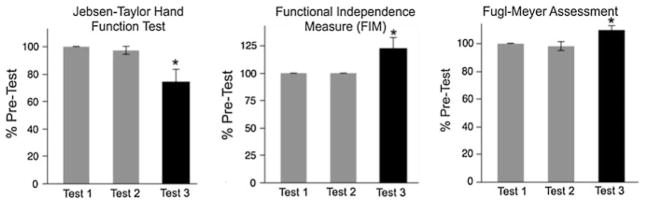
Brain lateralization is a ubiquitous feature of neural organization across the vertebrate spectrum. We have developed a model of motor lateralization that attributes different motor control processes to each cerebral hemisphere. This bilateral hemispheric model of motor control has successfully predicted hemisphere-specific motor control and motor learning deficits in the ipsilesional, or non-paretic, arm of patients with unilateral stroke. We now show across large number and range of stroke patients that these motor performance deficits in the non-paretic arm of stroke patients vary with both the side of the lesion, as well as with the severity of contralesional impairment. This last point can be functionally devastating for patients with severe contralesional paresis because for these individuals, performance of upper extremity activities of daily living depends primarily and often exclusively on ipsilesional arm function. We present a pilot study focused on improving the speed and coordination of ipsilesional arm function in a convenience sample of three stroke patients with severe contralesional impairment. Over a three-week period, patients received a total of nine 1.5 h sessions of training that included intense practice of virtual reality and real-life tasks. Our results indicated substantial improvements in ipsilesional arm movement kinematics, functional performance, and that these improvements carried over to improve functional independence. In addition, the contralesional arm improved in our measure of contralesional impairment, which was likely due to improved participation in activities of daily living. We discuss of our findings for physical rehabilitation.
Keywords: Bilateral hemispheric model; Contralesional; Dynamic dominance; Interlimb transfer; Ipsilesional; Jebsen-Taylor hand function test; Paresis; Rehabilitation.
Figures


References
-
- Bisazza A, Rogers LJ, Vallortigara G. The origins of cerebral asymmetry: a review of evidence of behavioural and brain lateralization in fishes, reptiles and amphibians. Neurosci Biobehav Rev. 1998;22:411–426. - PubMed
-
- Chestnut C, Haaland KY. Functional significance of ipsilesional motor deficits after unilateral stroke. Arch Phys Med Rehabil. 2008;89:62–68. - PubMed
-
- Desrosiers J, Bourbonnais D, Bravo G, Roy PM, Guay M. Performance of the ‘unaffected’ upper extremity of elderly stroke patients. Stroke. 1996;27:1564–1570. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
