

Role of Diastolic Stress Testing in the Evaluation for Heart Failure With Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study
- PMID: 28039229
- PMCID: PMC5330848
- DOI: 10.1161/CIRCULATIONAHA.116.024822
Role of Diastolic Stress Testing in the Evaluation for Heart Failure With Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study
Abstract
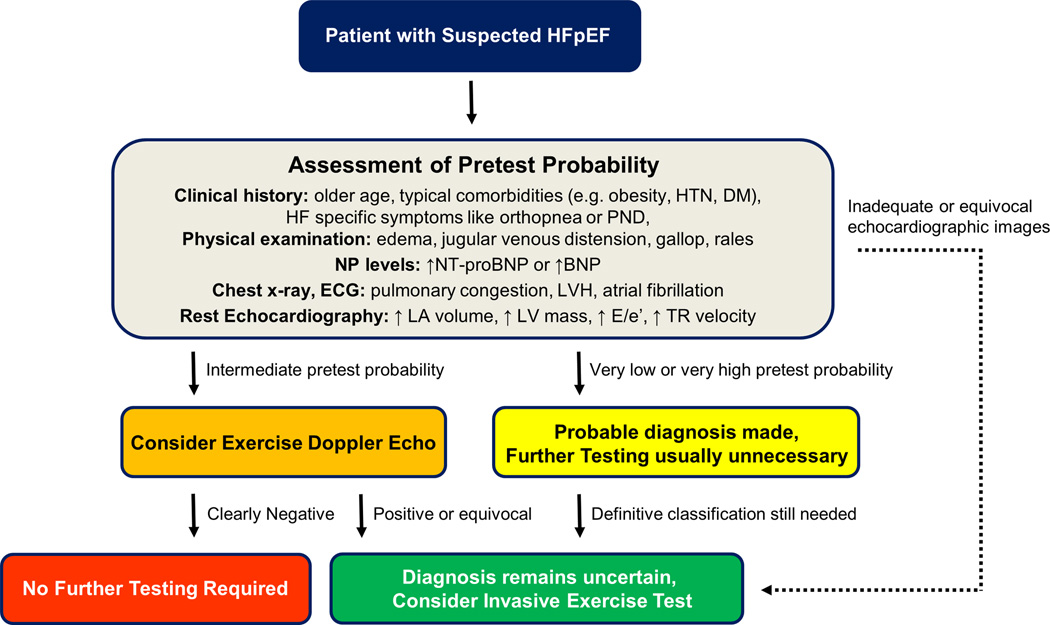
Background: Diagnosis of heart failure with preserved ejection fraction (HFpEF) is challenging and relies largely on demonstration of elevated cardiac filling pressures (pulmonary capillary wedge pressure). Current guidelines recommend use of natriuretic peptides (N-terminal pro-B type natriuretic peptide) and rest/exercise echocardiography (E/e' ratio) to make this determination. Data to support this practice are conflicting.
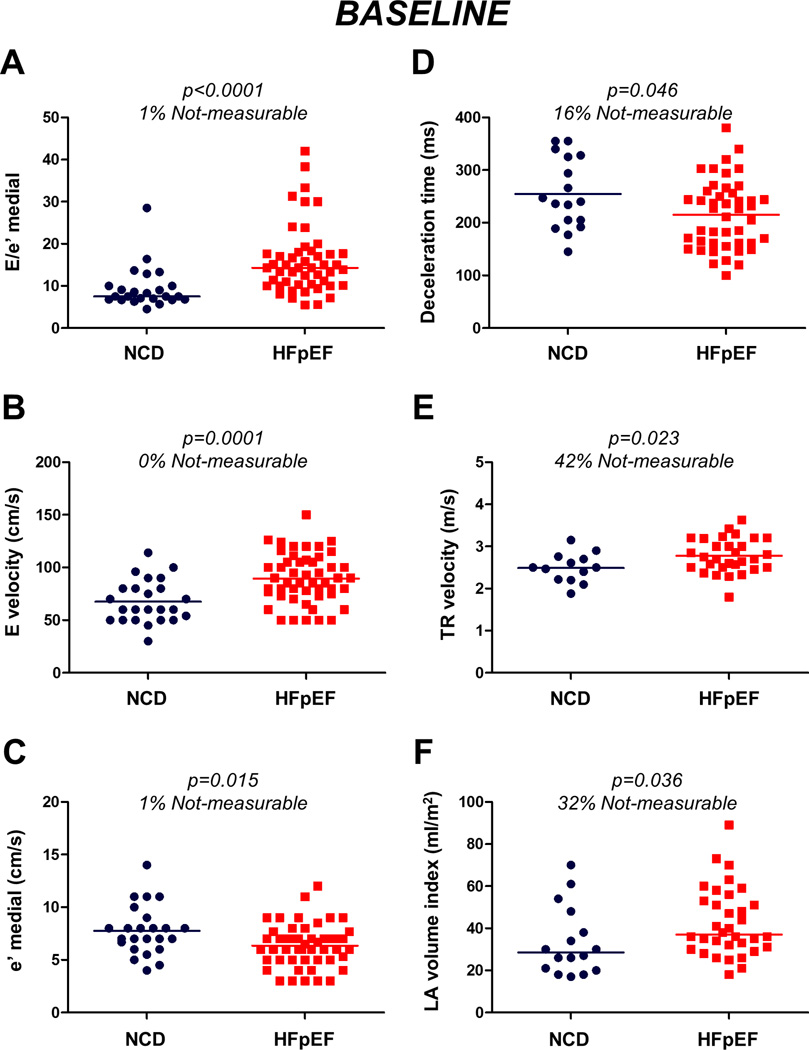
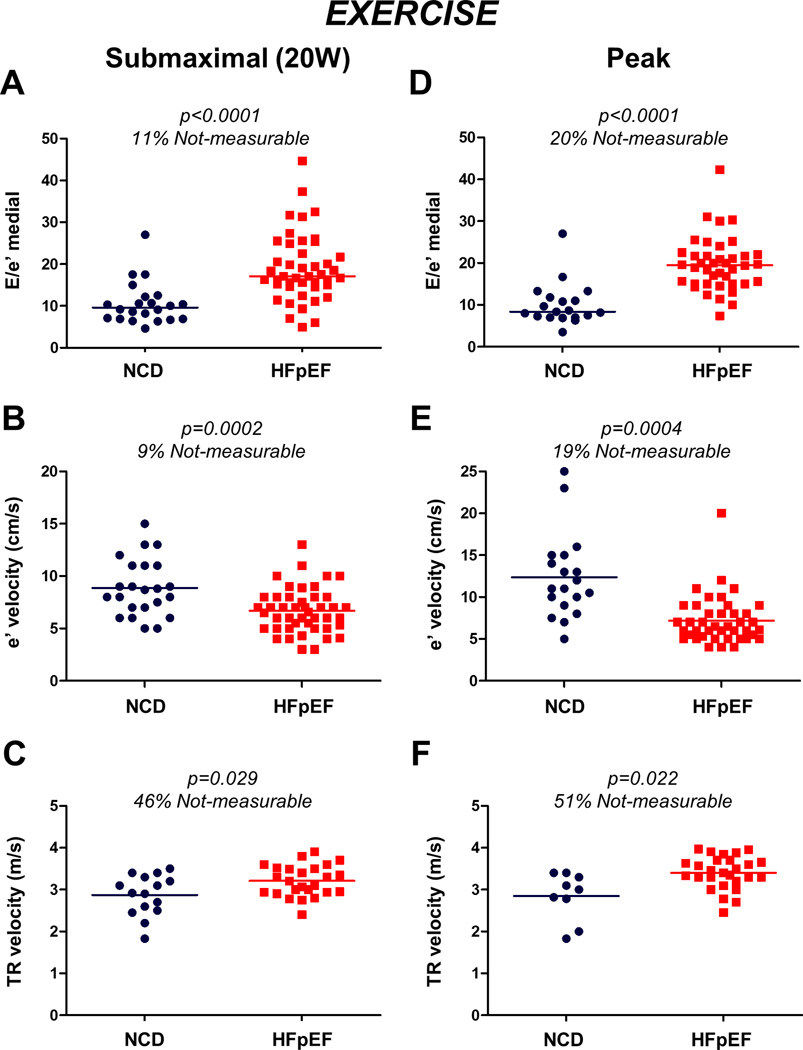
Methods: Simultaneous echocardiographic-catheterization studies were prospectively conducted at rest and during exercise in subjects with invasively proven HFpEF (n=50) and participants with dyspnea but no identifiable cardiac pathology (n=24).
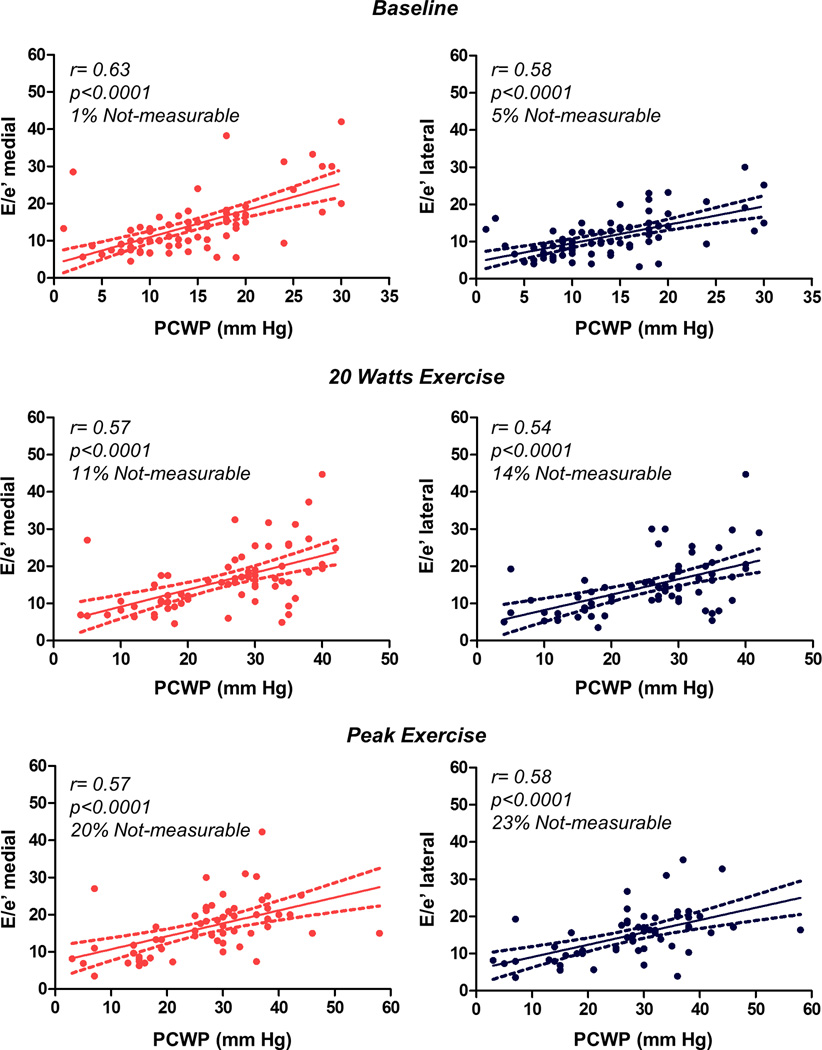
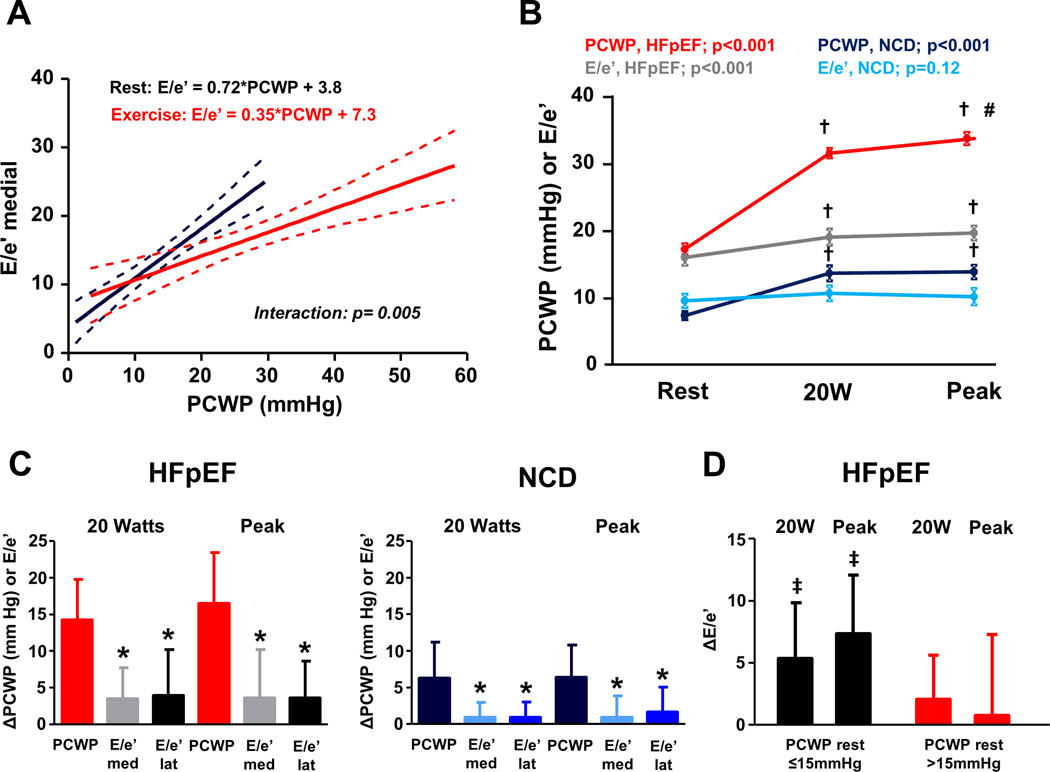
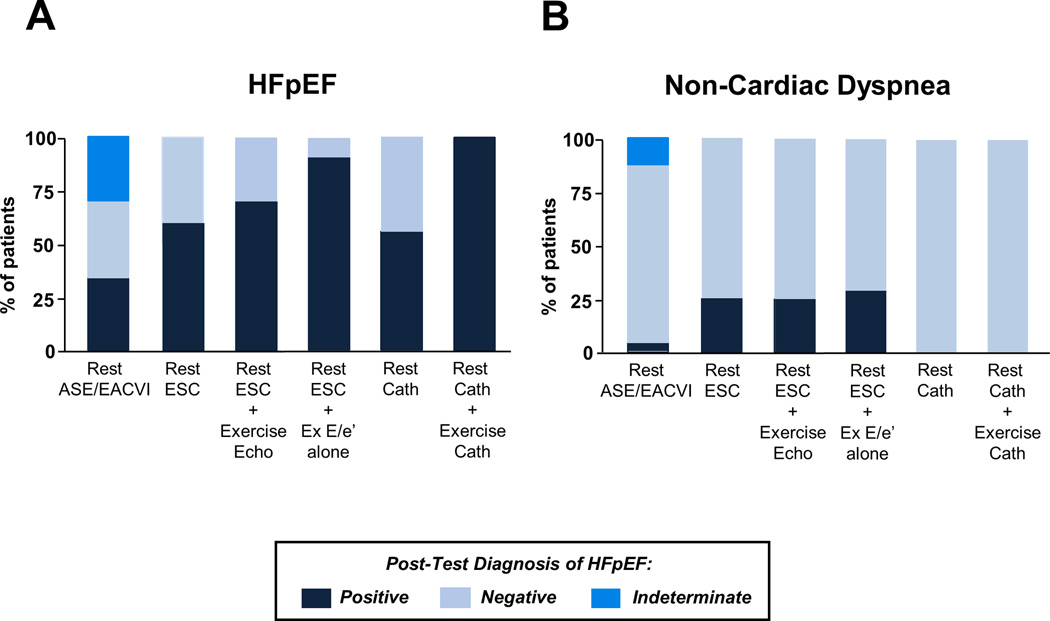
Results: N-Terminal pro-B type natriuretic peptide levels were below the level considered to exclude disease (≤125 pg/mL) in 18% of subjects with HFpEF. E/e' ratio was correlated with directly measured pulmonary capillary wedge pressure at rest (r=0.63, P<0.0001) and during exercise (r=0.57, P<0.0001). Although specific, current guidelines were poorly sensitive, identifying only 34% to 60% of subjects with invasively proven HFpEF on the basis of resting echocardiographic data alone. Addition of exercise echocardiographic data (E/e' ratio>14) improved sensitivity (to 90%) and thus negative predictive value, but decreased specificity (71%).
Conclusions: Currently proposed HFpEF diagnostic guidelines on the basis of resting data are poorly sensitive. Adding exercise E/e' data improves sensitivity and negative predictive value but compromises specificity, suggesting that exercise echocardiography may help rule out HFpEF. These results question the accuracy of current approaches to exclude HFpEF on the basis of resting data alone and reinforce the value of exercise testing using invasive and noninvasive hemodynamic assessments to definitively confirm or refute the diagnosis of HFpEF.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique Identifier: NCT01418248.
Keywords: diagnosis; exercise; exercise test; heart failure.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Letter by Smiseth and Nagueh et al Regarding Article, "Role of Diastolic Stress Testing in the Evaluation for Heart Failure With Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study".Circulation. 2017 Jul 25;136(4):428-429. doi: 10.1161/CIRCULATIONAHA.117.027881. Circulation. 2017. PMID: 28739815 No abstract available.
-
Response by Obokata and Borlaug to Letter Regarding Article, "Role of Diastolic Stress Testing in the Evaluation for Heart Failure With Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study".Circulation. 2017 Jul 25;136(4):430-431. doi: 10.1161/CIRCULATIONAHA.117.029037. Circulation. 2017. PMID: 28739816 Free PMC article. No abstract available.
References
-
- Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, Borbely A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG, Brutsaert DL. How to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the heart failure and echocardiography associations of the european society of cardiology. Eur Heart J. 2007;28:2539–2550. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 esc guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (esc) developed with the special contribution of the heart failure association (hfa) of the esc. Eur Heart J. 2016;37:2129–2200. - PubMed
-
- Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, 3rd, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, Marino P, Oh JK, Popescu BA, Waggoner AD. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the american society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiogr. 2016;29:277–314. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
