

Efficacy and safety results of ABT-414 in combination with radiation and temozolomide in newly diagnosed glioblastoma
- PMID: 28039367
- PMCID: PMC5570193
- DOI: 10.1093/neuonc/now257
Efficacy and safety results of ABT-414 in combination with radiation and temozolomide in newly diagnosed glioblastoma
Abstract
Background: The purpose of this study was to determine the maximum tolerated dose (MTD), recommended phase II dose (RPTD), safety, and pharmacokinetics of ABT-414 plus radiation and temozolomide in newly diagnosed glioblastoma. ABT-414 is a first-in-class, tumor-specific antibody-drug conjugate that preferentially targets tumors expressing overactive epidermal growth factor receptor (EGFR).
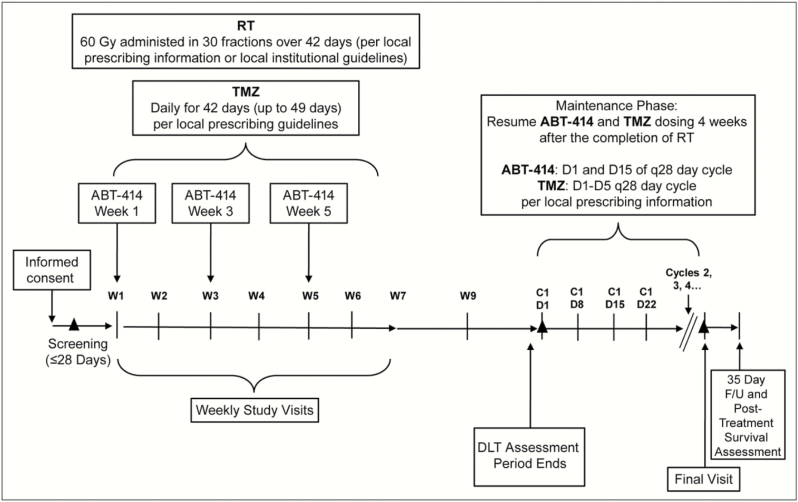
Methods: In this multicenter phase I study, patients received 0.5-3.2 mg/kg ABT-414 every 2 weeks by intravenous infusion. EGFR alterations, O6-methylguanine-DNA methyltransferase (MGMT) promoter hypermethylation, and isocitrate dehydrogenase (IDH1) gene mutations were assessed in patient tumors. Distinct prognostic classes were assigned to patients based on a Molecular Classification Predictor model.
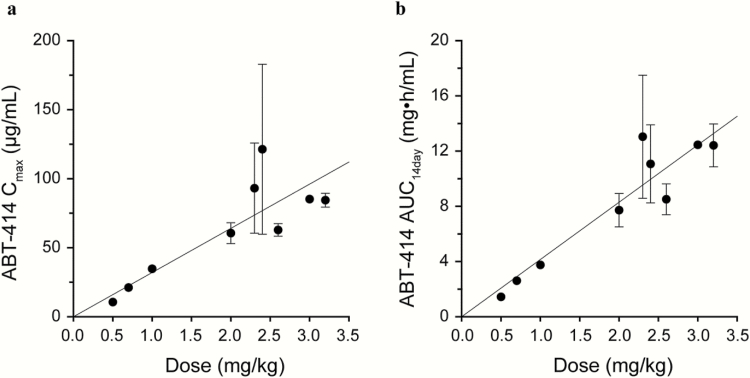
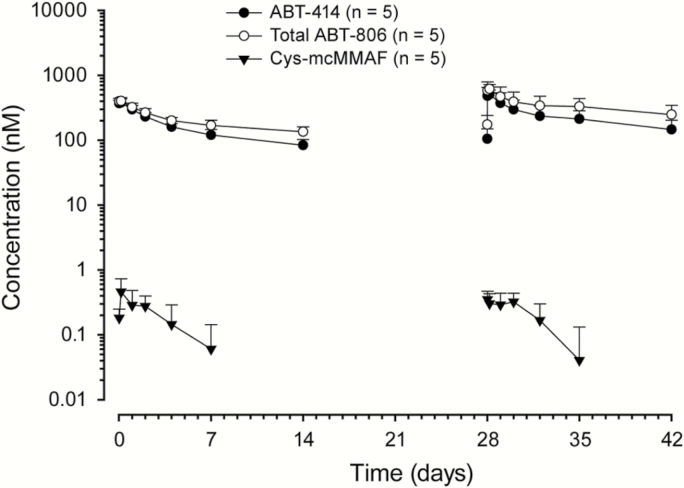
Results: As of January 7, 2016, forty-five patients were enrolled to receive ABT-414 plus radiation and temozolomide. The most common treatment emergent adverse events were ocular: blurred vision, dry eye, keratitis, photophobia, and eye pain. Ocular toxicity at any grade occurred in 40 patients and at grades 3/4 in 12 patients. RPTD and MTD were set at 2 mg/kg and 2.4 mg/kg, respectively. Among 38 patients with pretreatment tumor tested centrally, 39% harbored EGFR amplification, of which 73% had EGFRvIII mutation. Among patients with available tumor tissue (n = 30), 30% showed MGMT promoter methylation and none had IDH1 mutations. ABT-414 demonstrated an approximately dose proportional pharmacokinetic profile. The median duration of progression-free survival was 6.1 months; median overall survival has not been reached.
Conclusion: ABT-414 plus chemoradiation demonstrated an acceptable safety and pharmacokinetic profile in newly diagnosed glioblastoma. Randomized studies are ongoing to determine efficacy in newly diagnosed (NCT02573324) and recurrent glioblastoma (NCT02343406).
Keywords: ABT-414; EGFR; antibody-drug conjugate; glioblastoma; phase.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Stupp R, Taillibert S, Kanner AA, et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA. 2015;314(23):2535–2543. - PubMed
-
- Wick W, Brandes AA, Gorlia T, et al. Phase III trial exploring the combination of bevacizumab and lomustine in patients with first recurrence of a glioblastoma: the EORTC 26101 trial. Neuro Oncol. 2015;17 (suppl 5): v1.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
