

Pathway from Delirium to Death: Potential In-Hospital Mediators of Excess Mortality
- PMID: 28039852
- PMCID: PMC5435507
- DOI: 10.1111/jgs.14743
Pathway from Delirium to Death: Potential In-Hospital Mediators of Excess Mortality
Abstract
Objectives: (1) To determine the relationship of incident delirium during hospitalization with 90-day mortality; (2) to identify potential in-hospital mediators through which delirium increases 90-day mortality.
Design: Analysis of data from Project Recovery, a controlled clinical trial of a delirium prevention intervention from 1995 to 1998 with follow-up through 2000.
Setting: Large academic hospital.
Participants: Patients ≥70 years old without delirium at hospital admission who were at intermediate-to-high risk of developing delirium and received usual care only.
Measurements: (1) Incident delirium; (2) potential mediators of delirium on death including use of restraining devices (physical restraints, urinary catheters), development of hospital acquired conditions (HACs) (falls, pressure ulcers), and exposure to other noxious insults (sleep deprivation, acute malnutrition, dehydration, aspiration pneumonia); (3) death within 90 days of admission.
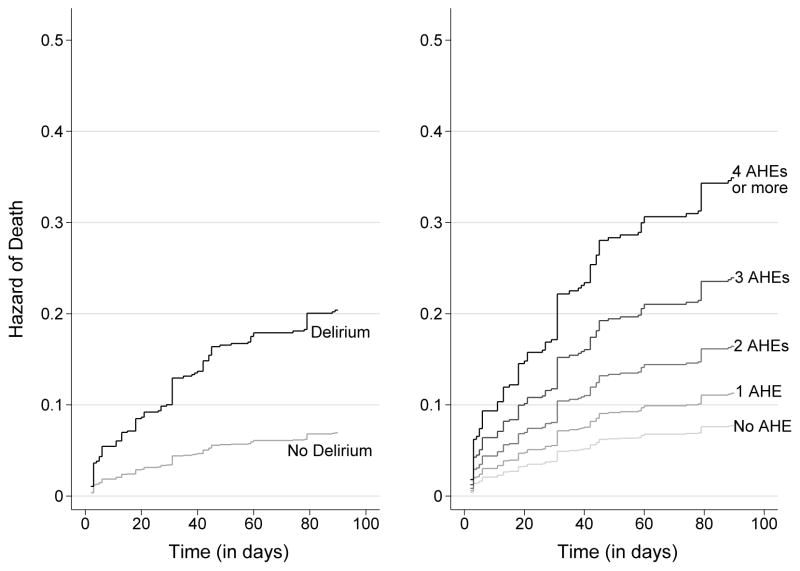
Results: Among 469 patients, 70 (15%) developed incident delirium. These patients were more likely to experience restraining devices (37% vs 16%, P < .001), HACs (37% vs 12%, P < .001), other noxious insults (63% vs 49%, P = .03), and 90-day mortality (24% vs 6%, P < .001). The inverse probability weighted hazard of death due to delirium was 4.2 (95% CI = 2.8-6.3) in bivariable analyses, increased in a graded manner with additional exposures to restraining devices, HACs, and other noxious insults, and declined by 10.9% after addition of these potential mediator categories, providing evidence of mediation.
Conclusion: Restraining devices, HACs, and additional noxious insults were more frequent among patients with delirium, increased mortality in a graded manner, and were responsible for a significant percentage of the association of delirium with death. Additional efforts to prevent potential downstream mediators through which delirium increases mortality may help to improve outcomes among hospitalized older adults.
Keywords: delirium; geriatrics; hospital care; hospital-acquired conditions; quality of care.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Figures
References
-
- Eeles EM, Hubbard RE, White SV, et al. Hospital use, institutionalisation and mortality associated with delirium. Age Ageing. 2010;39:470–475. - PubMed
-
- Shehabi Y, Riker RR, Bokesch PM, et al. Delirium duration and mortality in lightly sedated, mechanically ventilated intensive care patients. Crit Care Med. 2010;38:2311–2318. - PubMed
-
- Oldenbeuving AW, de Kort PL, Jansen BP, et al. Delirium in the acute phase after stroke: incidence, risk factors, and outcome. Neurology. 2011;76:993–999. - PubMed
-
- Ansaloni L, Catena F, Chattat R, et al. Risk factors and incidence of postoperative delirium in elderly patients after elective and emergency surgery. Br J Surg. 2010;97:273–280. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
