

Prognostic Value of BRAF and KRAS Mutations in MSI and MSS Stage III Colon Cancer
- PMID: 28040692
- PMCID: PMC6075212
- DOI: 10.1093/jnci/djw272
Prognostic Value of BRAF and KRAS Mutations in MSI and MSS Stage III Colon Cancer
Abstract
Background: The prognostic value of BRAF and KRAS mutations within microsatellite-unstable (MSI) and microsatellite-stable (MSS) subgroups of resected colon carcinoma patients remains controversial. We examined this question in prospectively collected biospecimens from stage III colon cancer with separate analysis of MSI and MSS tumors from patients receiving adjuvant FOLFOX +/- cetuximab in two adjuvant therapy trials.
Methods: Three groups were defined: BRAF Mutant, KRAS Mutant, and double wild-type. The analytic strategy involved estimation of study-specific effects, assessment of homogeneity of results, and then analysis of pooled data as no differences in patient outcome were found between treatment arms in both trials. Associations of mutations with patient outcome were analyzed, and multivariable models were adjusted for treatment and relevant factors.
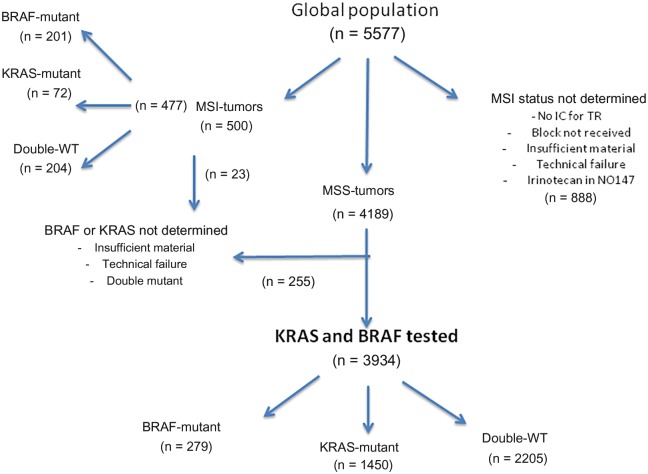
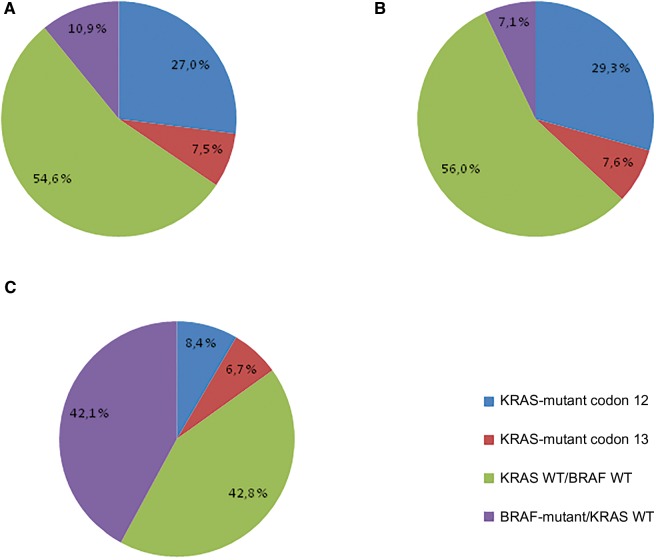
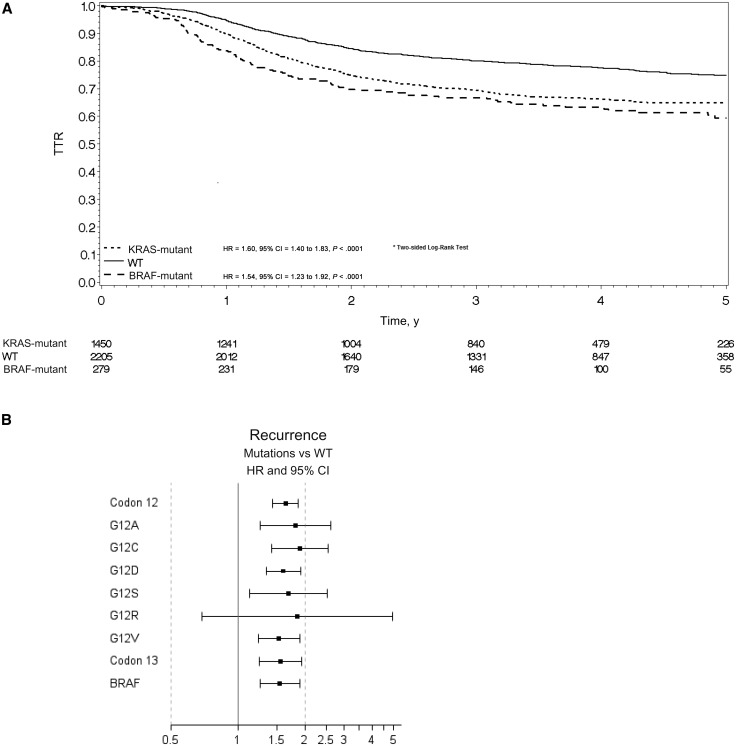
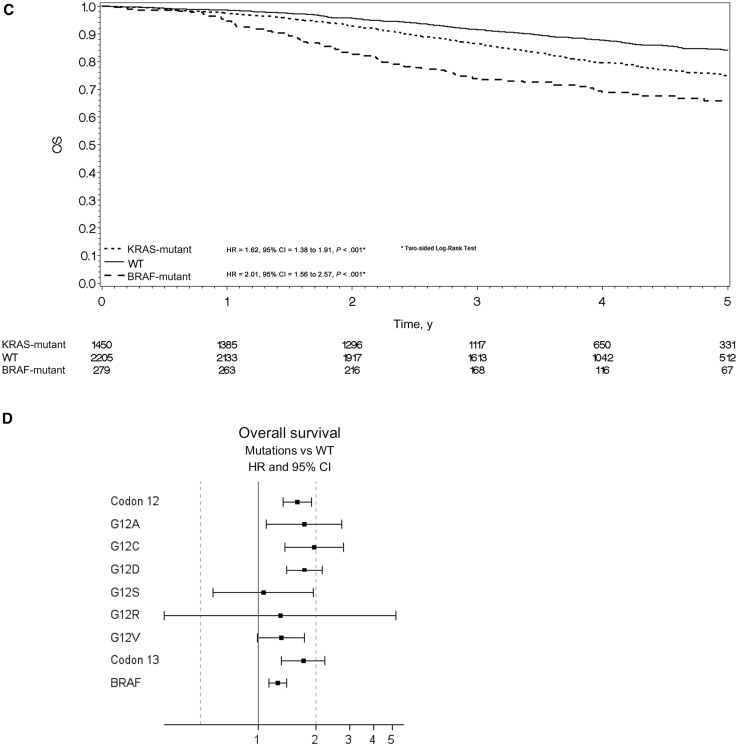
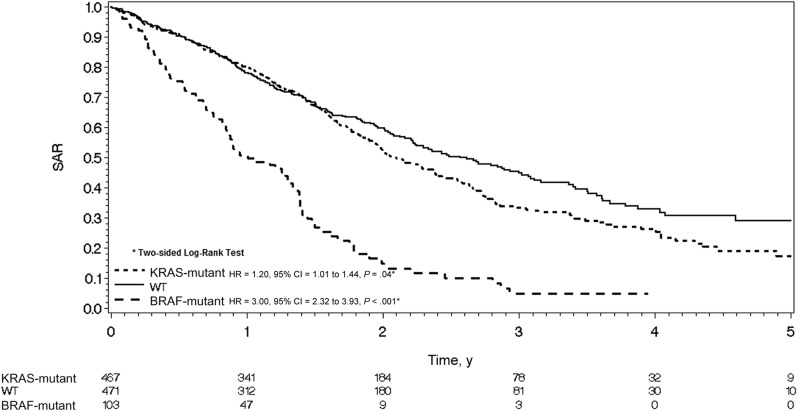
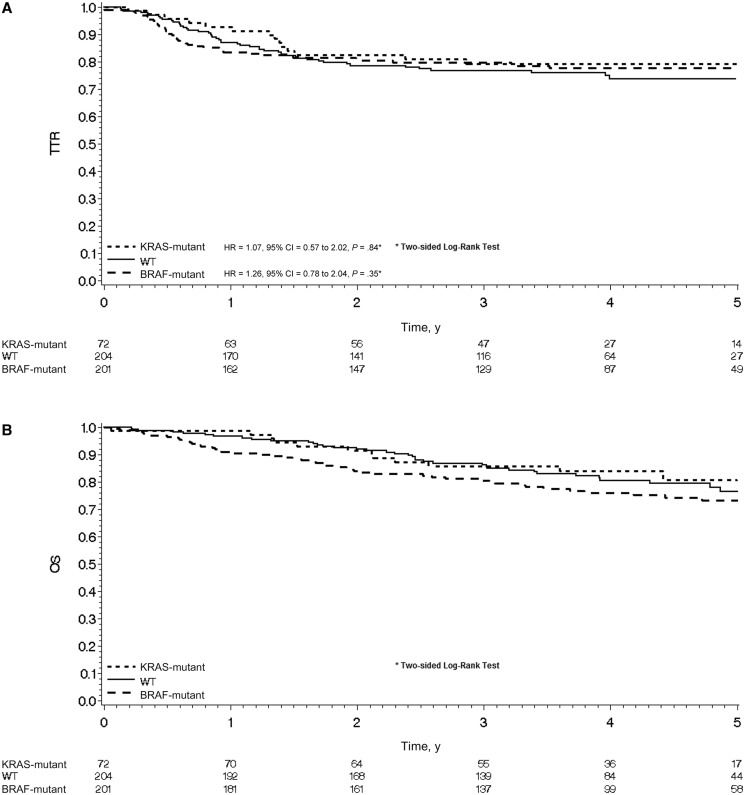
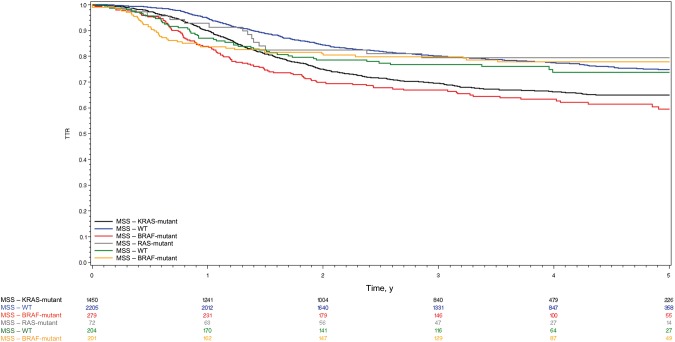
Results: Four thousand four hundred eleven tumors were evaluable for BRAF and KRAS mutations and mismatch repair status; 3934 were MSS and 477 were MSI. In MSS patients, all BRAF V600E mutations (hazard ratio [HR] = 1.54, 95% confidence interval [CI] = 1.23 to 1.92, P < .001), KRAS codon 12 alterations, and p.G13D mutations (HR = 1.60, 95% CI = 1.40 to 1.83, P < .001) were associated with shorter time to recurrence (TTR) and shorter survival after relapse (SAR; HR = 3.02 , 95% CI = 2.32 to 3.93, P < .001, and HR = 1.20, 95% CI = 1.01 to 1.44, P = .04, respectively). Overall survival (OS) in MSS patients was poorer for BRAF-mutant patients (HR = 2.01, 95% CI = 1.56 to 2.57, P < .001) and KRAS-mutant patients (HR = 1.62, 95% CI = 1.38 to 1.91, P < .001) vs wild-type. No prognostic role of KRAS or BRAF mutations was seen in MSI patients. Furthermore, no interaction was found between treatment arm (with or without cetuximab) and KRAS and BRAF mutations for TTR or OS in MSS patients.
Conclusions: In a pooled analysis of resected stage III colon cancer patients receiving adjuvant FOLFOX, BRAF or KRAS mutations are independently associated with shorter TTR, SAR, and OS in patients with MSS, but not MSI, tumors. Future clinical trials in the adjuvant setting should consider these mutations as important stratification factors.
© The Author 2016. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71–96. - PubMed
-
- Benson AB 3rd, Venook AP, Bekaii-Saab T, et al. Colon cancer, version 3.2014. J Natl Compr Canc Netw. 2014;12(7):1028–1059. - PubMed
-
- Van Cutsem E, Cervantes A, Nordlinger B, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(suppl 3):iii1–iii9. - PubMed
-
- Bokemeyer C, Bondarenko I, Hartmann JT, et al. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: The OPUS study. Ann Oncol. 2011;22(7):1535–1546. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
