

Recommendations for Clinical Trial Development in Mantle Cell Lymphoma
- PMID: 28040733
- PMCID: PMC6059122
- DOI: 10.1093/jnci/djw263
Recommendations for Clinical Trial Development in Mantle Cell Lymphoma
Abstract
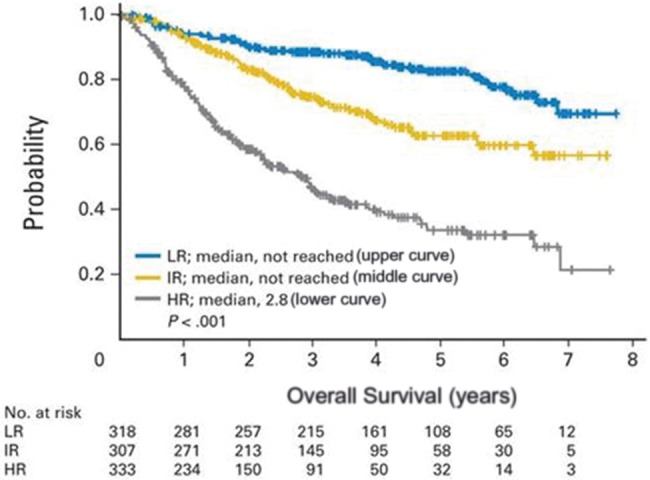
Mantle cell lymphoma (MCL) comprises around 6% of all non-Hodgkin's lymphoma (NHL) diagnoses. In younger patients, age less than 60 to 65 years, aggressive induction often followed by consolidation with autologous stem cell transplant has suggested improved outcomes in this population. Less intensive therapies in older patients often followed by maintenance have been studied or are under active investigation. However, despite recent advances, MCL remains incurable, with a median overall survival of around five years. Patients with high-risk disease have particularly poor outcomes. Treatment varies widely across institutions, and to date no randomized trials comparing intensive vs less intensive approaches have been reported. Although recent data have highlighted the heterogeneity of MCL outcomes, patient assessment for treatment selection has largely been driven by patient age with little regard to fitness, disease biology, or disease risk. One critical advance is the finding that minimal residual disease status (MRD) after induction correlates with long-term outcomes. As such, its use as a potential end point could inform clinical trial design. In order to more rapidly improve the outcomes of MCL patients, clinical trials are needed that prospectively stratify patients on the basis of MCL biology and disease risk, incorporate novel agents, and use MRD to guide the need for additional therapy.
Published by Oxford University Press 2016. This work is written by US Government employees and is in the public domain in the US.
Figures
References
-
- Zhou Y, Wang H, Fang W, et al. Incidence trends of mantle cell lymphoma in the United States between 1992 and 2004. Cancer. 2008;113(4):791–798. - PubMed
-
- Harris NL, Jaffe ES, Stein H, et al. A revised European-American classification of lymphoid neoplasms: A proposal from the international lymphoma study group. Blood. 1994;84(5):1361–1392. - PubMed
-
- Chandran R, Gardiner S, Simon M, Spurgeon SE. Survival trends in mantle cell lymphoma in the United States over 16 years 1992-2007. Leuk Lymph. 2012;53(8):1488–1493. - PubMed
-
- Herrmann A, Hoster E, Zwingers T, et al. Improvement of overall survival in advanced stage mantle cell lymphoma. J Clin Oncol. 2009;27(4):511–518. - PubMed
-
- Schmidt C, Dreyling M. Therapy of mantle cell lymphoma: Current standards and future strategies. Hematol Oncol Clin North Am. 2008;22(5):953–963. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
