

The impact of histology and delivered dose on local control of spinal metastases treated with stereotactic radiosurgery
- PMID: 28041329
- PMCID: PMC5568686
- DOI: 10.3171/2016.9.FOCUS16369
The impact of histology and delivered dose on local control of spinal metastases treated with stereotactic radiosurgery
Abstract
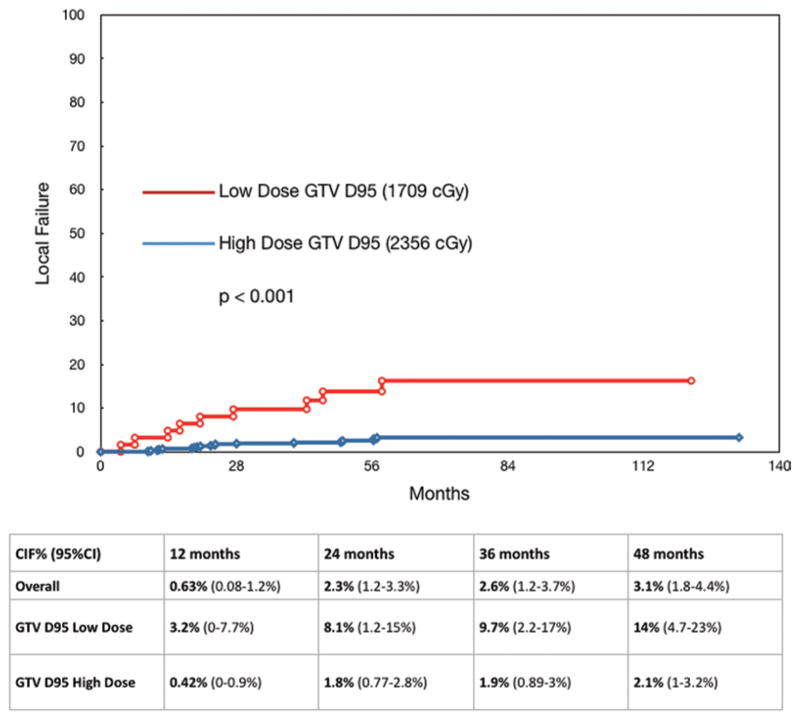
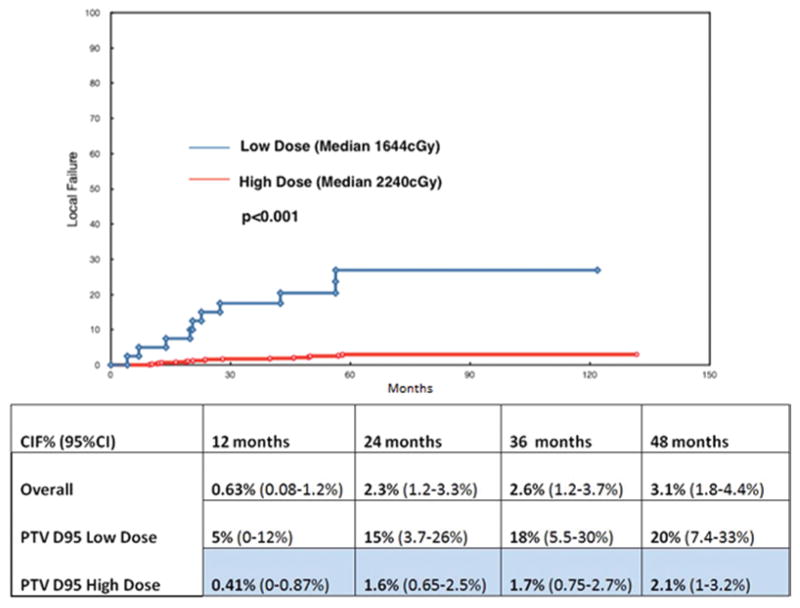
OBJECTIVE An analysis of factors contributing to durable radiographic control of spinal metastases was undertaken, drawing from a large single-institution database in an attempt to elucidate indications and dose requirements for successful treatment. METHODS All patients treated at a single institution with stereotactic radiosurgery (SRS) of the spine as first-line therapy were assessed for local progression of the treated site, defined as radiographic enlargement of the treated tumor and/or biopsy-proven evidence of active tumor cells. All patients were followed with CT, PET, or MR imaging every 3-6 months until death. Treatment decisions were made by a multidisciplinary team of radiation oncologists, neurosurgeons, and neuroradiologists. Target volumes were defined according to the international consensus guidelines and were reviewed in a multidisciplinary conference. Image-guided techniques and intensity modulation were used for every case. The tumor's histological type, gross tumor volume (GTV), dose that covers 95% of the GTV (GTV D95), percentage of GTV covered by 95% of the prescribed dose (GTV V95), planning target volume (PTV), dose that covers 95% of the PTV (PTV D95), and percentage of PTV covered by 95% of the prescribed dose (PTV V95) were analyzed for significance in relation to local control, based on time to local progression. RESULTS A total of 811 lesions were treated in 657 patients between 2003 and 2015 at a single institution. The mean follow-up and overall survival for the entire cohort was 26.9 months (range 2-141 months). A total of 28 lesions progressed and the mean time to failure was 26 months (range 9.7-57 months). The median prescribed dose was 2400 cGy (range 1600-2600 cGy). Both GTV D95 and PTV D95 were highly significantly associated with local failure in univariate analysis, but GTV and PTV and histological type did not reach statistical significance. The median GTV D95 for the cohort equal to or above the GTV D95 1830 cGy cut point (high dose) was 2356 cGy, and it was 1709 cGy for the cohort of patients who received less than 1830 cGy (low dose). In terms of PTV D95, the median dose for those equal to or above the cut point of 1740 cGy (high dose) was 2233 cGy, versus 1644 cGy for those lesions below the PTV D95 cut point of 1740 cGy (low dose). CONCLUSIONS High-dose single-session SRS provides durable long-term control, regardless of the histological findings or tumor size. In this analysis, the only significant factors predictive of local control were related to the actual dose of radiation given. Although the target volumes were well treated with the intended dose, those lesions irradiated to higher doses (median GTV D95 2356 cGy, minimum 1830 cGy) had a significantly higher probability of durable local control than those treated with lower doses (median PTV D95 2232 cGy, minimum of 1740 cGy) (p < 0.001). Patients in the high-dose cohort had a 2% cumulative rate of local failure. Histological findings were not associated with local failure, suggesting that radioresistant histological types benefit in particular from radiosurgery. For patients with a favorable prognosis, a higher dose of SRS is important for long-term outcomes.
Keywords: CIF = cumulative incidence of local failure; CTV = clinical target volume; GTV = gross tumor volume; GTV D95 = dose that covers 95% of the GTV; GTV V95 = percentage of GTV covered by 95% of the prescribed dose; PTV = planning target volume; PTV D95 = dose that covers 95% of the PTV; PTV V95 = percentage of PTV covered by 95% of the prescribed dose; SRS = stereotactic radiosurgery; local control; spinal metastases; stereotactic radiosurgery.
Figures
References
-
- Bate BG, Khan NR, Kimball BY, Gabrick K, Weaver J. Stereotactic radiosurgery for spinal metastases with or without separation surgery. J Neurosurg Spine. 2015;22:409–415. - PubMed
-
- Chan NK, Abdullah KG, Lubelski D, Steinmetz MP, Benzel EC, Shin JH, et al. Stereotactic radiosurgery for metastatic spine tumors. J Neurosurg Sci. 2014;58:37–44. - PubMed
-
- Cox BW, Spratt DE, Lovelock M, Bilsky MH, Lis E, Ryu S, et al. International Spine Radiosurgery Consortium consensus guidelines for target volume definition in spinal stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2012;83:e597–e605. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
