

Novel implications in the treatment of hepatocellular carcinoma
- PMID: 28042235
- PMCID: PMC5198244
- DOI: 10.20524/aog.2016.0092
Novel implications in the treatment of hepatocellular carcinoma
Abstract
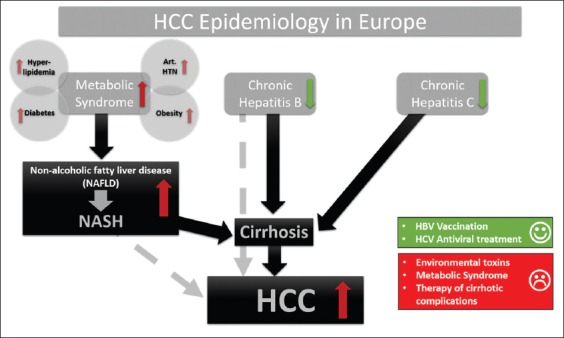
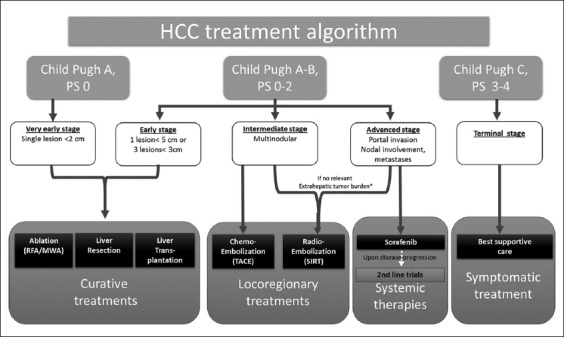
Worldwide hepatocellular carcinoma remains one of the leading causes of cancer-related death, associated with a poor prognosis due to late diagnosis in the majority of cases. Physicians at care are frequently confronted with patients who are ineligible for curative treatment such as liver resection, transplantation or radiofrequency ablation. Besides established palliative locoregional therapies, such as ablation or chemoembolization, new treatment options, such as microwave ablation, drug-eluting bead transarterial chemoembolization or selective internal radiation therapy, are emerging; however, data from randomized controlled trials are still lacking. In order to achieve optimal tumor control, patients should receive tailored treatment concepts, considering their tumor burden, liver function and performance status, instead of strictly assigning patients to treatment modalities following algorithms that may be partly very restrictive. Palliative locoregional pretreatment might facilitate downstaging to ensure later curative resection or transplantation. In addition, the combined utilization of different locoregional treatment options or systemic co-treatment has been the subject of several trials. In cases where local tumor control cannot be achieved, or in the scenario of extrahepatic spread, sorafenib remains the only approved systemic therapy option. Alternative targeted therapies, such as immune checkpoint inhibitors have shown encouraging preliminary results, while data from phase III studies are pending.
Keywords: Hepatocellular carcinoma; individualized treatment concept; liver surgery; locoregional therapy; systemic therapy.
Conflict of interest statement
Conflict of Interest: Jan Best, Jens M. Theysohn, Alexander Dechêne, Stefan Müller: Speaker honoraria and advisory board meetings BTG Intl.; Jan Best: Travel grant Bayer; Alexander Dechêne: Speaker honoraria and advisory board meetings Bayer
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide:sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Berhane S, Toyoda H, Tada T, et al. Role of the GALAD and BALAD-2 serologic models in diagnosis of hepatocellular carcinoma and prediction of survival in patients. Clin Gastroenterol Hepatol. 2016;14:875–886. - PubMed
-
- Johnson PJ, Pirrie SJ, Cox TF, et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol Biomarkers Prev. 2014;23:144–153. - PubMed
-
- Ertle J, Dechêne A, Sowa JP, et al. Non-alcoholic fatty liver disease progresses to hepatocellular carcinoma in the absence of apparent cirrhosis. Int J Cancer. 2011;128:2436–2443. - PubMed
-
- Romagnoli R, Mazzaferro V, Bruix J. Surgical resection for hepatocellular carcinoma: Moving from what can be done to what is worth doing. Hepatology. 2015;62:340–342. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources