

In Patients With Severe Alcoholic Hepatitis, Prednisolone Increases Susceptibility to Infection and Infection-Related Mortality, and Is Associated With High Circulating Levels of Bacterial DNA
- PMID: 28043903
- PMCID: PMC6381387
- DOI: 10.1053/j.gastro.2016.12.019
In Patients With Severe Alcoholic Hepatitis, Prednisolone Increases Susceptibility to Infection and Infection-Related Mortality, and Is Associated With High Circulating Levels of Bacterial DNA
Abstract
Background & aims: Infections are common in patients with severe alcoholic hepatitis (SAH), but little information is available on how to predict their development or their effects on patients. Prednisolone is advocated for treatment of SAH, but can increase susceptibility to infection. We compared the effects of infection on clinical outcomes of patients treated with and without prednisolone, and identified risk factors for development of infection in SAH.
Methods: We analyzed data from 1092 patients enrolled in a double-blind placebo-controlled trial to evaluate the efficacy of treatment with prednisolone (40 mg daily) or pentoxifylline (400 mg 3 times each day) in patients with SAH. The 2 × 2 factorial design led to 547 patients receiving prednisolone; 546 were treated with pentoxifylline. The trial was conducted in the United Kingdom from January 2011 through February 2014. Data on development of infection were collected at evaluations performed at screening, baseline, weekly during admission, on discharge, and after 90 days. Patients were diagnosed with infection based on published clinical and microbiologic criteria. Risk factors for development of infection and effects on 90-day mortality were evaluated separately in patients treated with prednisolone (n = 547) and patients not treated with prednisolone (n = 545) using logistic regression. Pretreatment blood levels of bacterial DNA (bDNA) were measured in 731 patients.
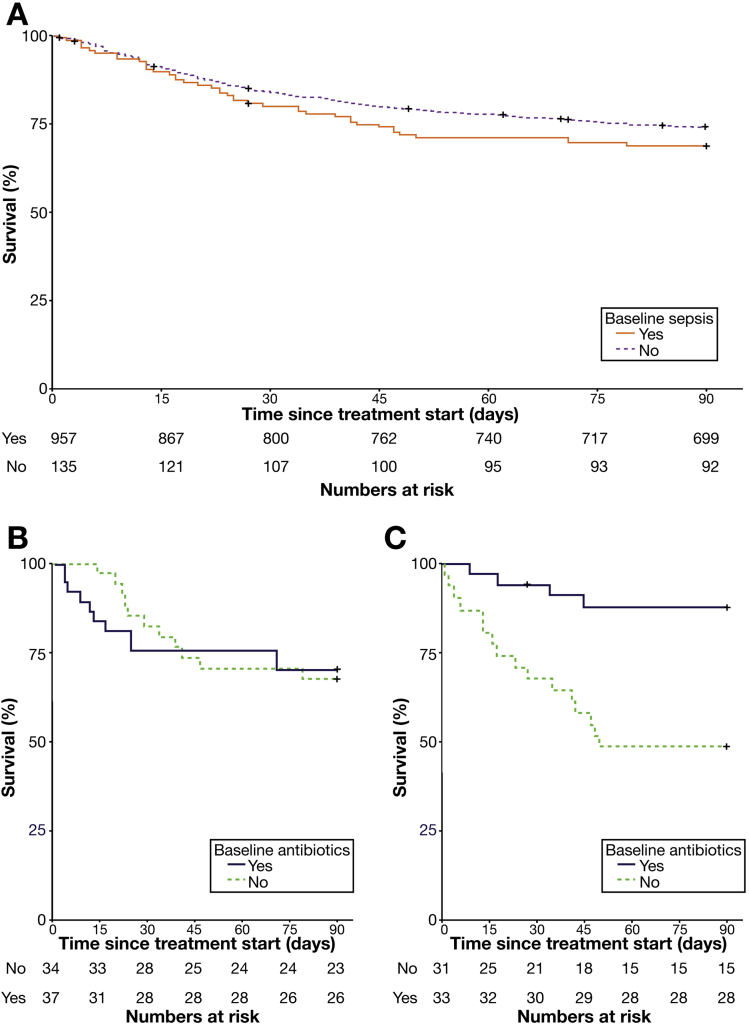
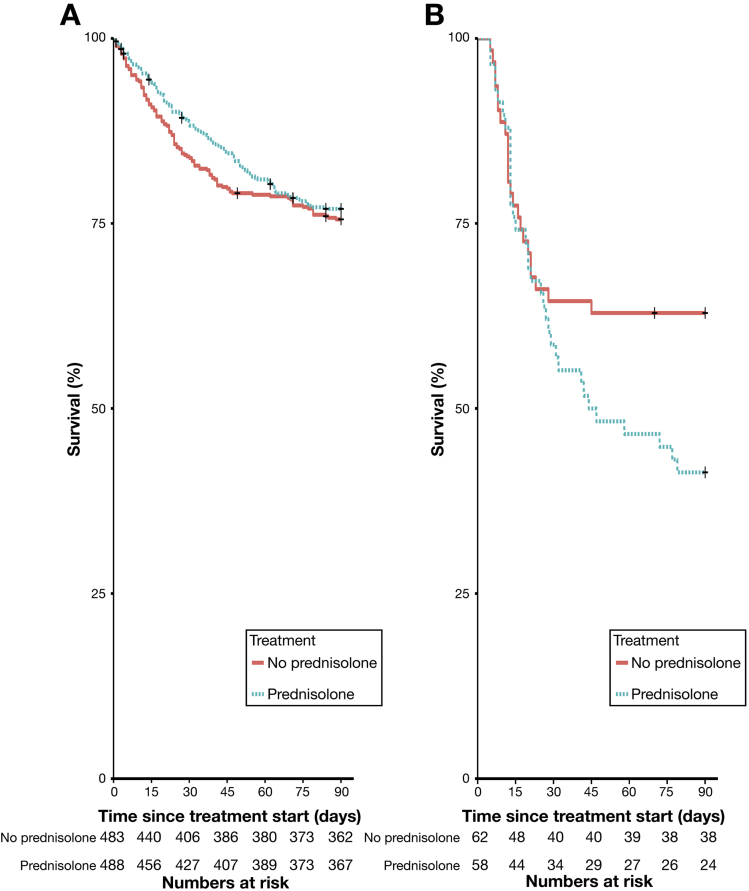
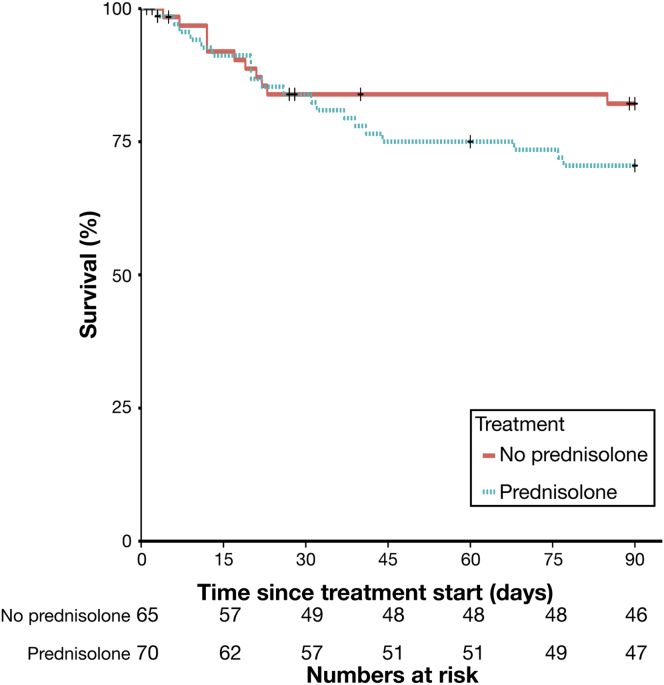
Results: Of the 1092 patients in the study, 135 had an infection at baseline, 251 developed infections during treatment, and 89 patients developed an infection after treatment. There was no association between pentoxifylline therapy and the risk of serious infection (P = .084), infection during treatment (P = .20), or infection after treatment (P = .27). Infections classified as serious were more frequent in patients treated with prednisolone (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.27-2.92; P = .002). There was no association between prednisolone therapy and infection during treatment (OR, 1.04; 95% CI, 0.78-1.37; P = .80). However, a higher proportion (10%) of patients receiving prednisolone developed an infection after treatment than of patients not given prednisolone (6%) (OR, 1.70; 95% CI, 1.07-2.69; P = .024). Development of infection was associated with increased 90-day mortality in patients with SAH treated with prednisolone, independent of model for end-stage liver disease or Lille score (OR, 2.46; 95% CI, 1.41-4.30; P = .002). High circulating bDNA predicted infection that developed within 7 days of prednisolone therapy, independent of Model for End-Stage Liver Disease and white blood cell count (OR, 4.68; 95% CI, 1.80-12.17; P = .001). In patients who did not receive prednisolone, infection was not independently associated with 90-day mortality (OR, 0.94; 95% CI, 0.54-1.62; P = .82) or levels of bDNA (OR, 0.83; 95% CI, 0.39-1.75; P = .62).
Conclusions: Patients with SAH given prednisolone are at greater risk for developing serious infections and infections after treatment than patients not given prednisolone, which may offset its therapeutic benefit. Level of circulating bDNA before treatment could identify patients at high risk of infection if given prednisolone; these data could be used to select therapies for patients with SAH. EudraCT no: 2009-013897-42; Current Controlled Trials no: ISRCTN88782125.
Keywords: E coli; MELD; STOPAH Trial; Steroid.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Alcoholic liver disease: Alcoholic hepatitis: a warning for prednisolone and infection risk?Nat Rev Gastroenterol Hepatol. 2017 Feb;14(2):68. doi: 10.1038/nrgastro.2017.5. Epub 2017 Jan 18. Nat Rev Gastroenterol Hepatol. 2017. PMID: 28096540 No abstract available.
-
Infection in Severe Alcoholic Hepatitis: Yet Another Piece in the Puzzle.Gastroenterology. 2017 Apr;152(5):938-940. doi: 10.1053/j.gastro.2017.02.030. Epub 2017 Mar 1. Gastroenterology. 2017. PMID: 28259797 No abstract available.
-
Circulating levels of bacterial DNA and risk of infections in severe alcoholic hepatitis.Clin Res Hepatol Gastroenterol. 2017 Sep;41(4):354-356. doi: 10.1016/j.clinre.2017.06.001. Epub 2017 Jul 24. Clin Res Hepatol Gastroenterol. 2017. PMID: 28750768 No abstract available.
References
-
- Maddrey W.C., Boitnott J.K., Bedine M.S. Corticosteroid therapy of alcoholic hepatitis. Gastroenterology. 1978;75:193–199. - PubMed
-
- Mathurin P., O’Grady J., Carithers R.L. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis: meta-analysis of individual patient data. Gut. 2011;60:255–260. - PubMed
-
- Thursz M.R., Richardson P., Allison M. Prednisolone or pentoxifylline for alcoholic hepatitis. N Engl J Med. 2015;372:1619–1628. - PubMed
-
- Louvet A., Wartel F., Castel H. Infection in patients with severe alcoholic hepatitis treated with steroids: early response to therapy is the key factor. Gastroenterology. 2009;137:541–548. - PubMed
-
- European Association for the Study of Liver Diseases EASL Clinical Practical Guidelines: management of alcoholic liver disease. J Hepatol. 2012;57:399–420. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
