

An abnormal periventricular magnetization transfer ratio gradient occurs early in multiple sclerosis
- PMID: 28043954
- PMCID: PMC5841055
- DOI: 10.1093/brain/aww296
An abnormal periventricular magnetization transfer ratio gradient occurs early in multiple sclerosis
Abstract
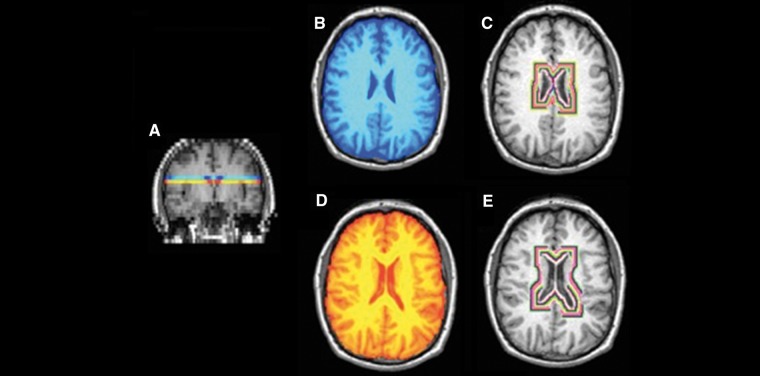
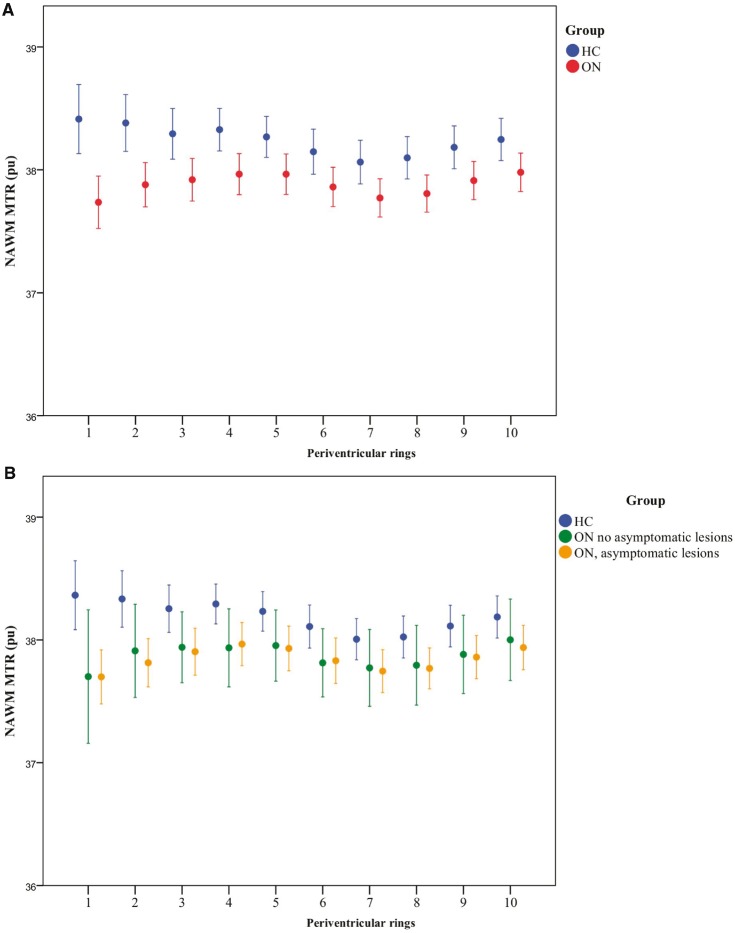
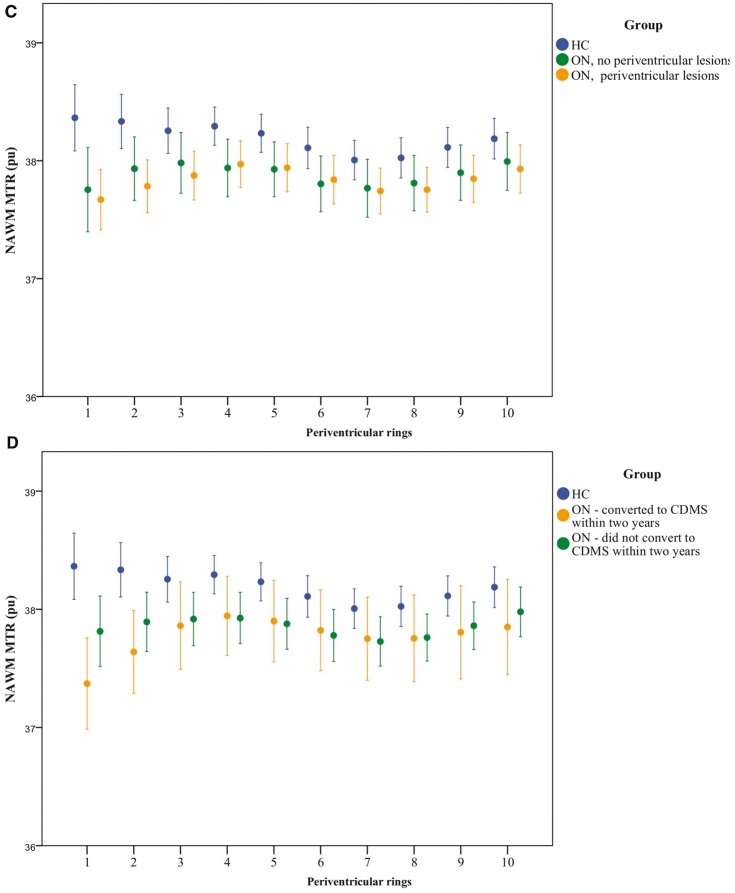
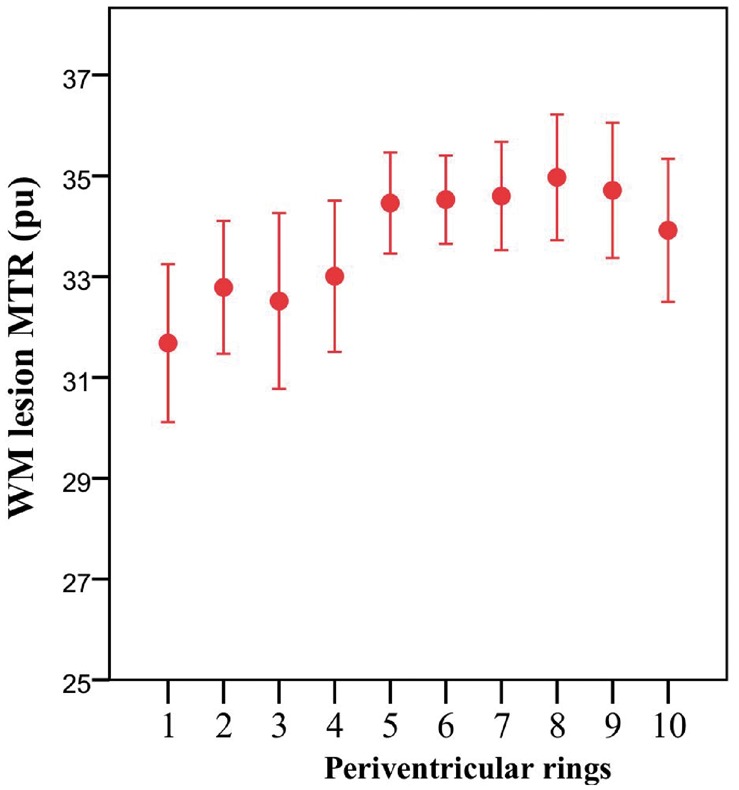
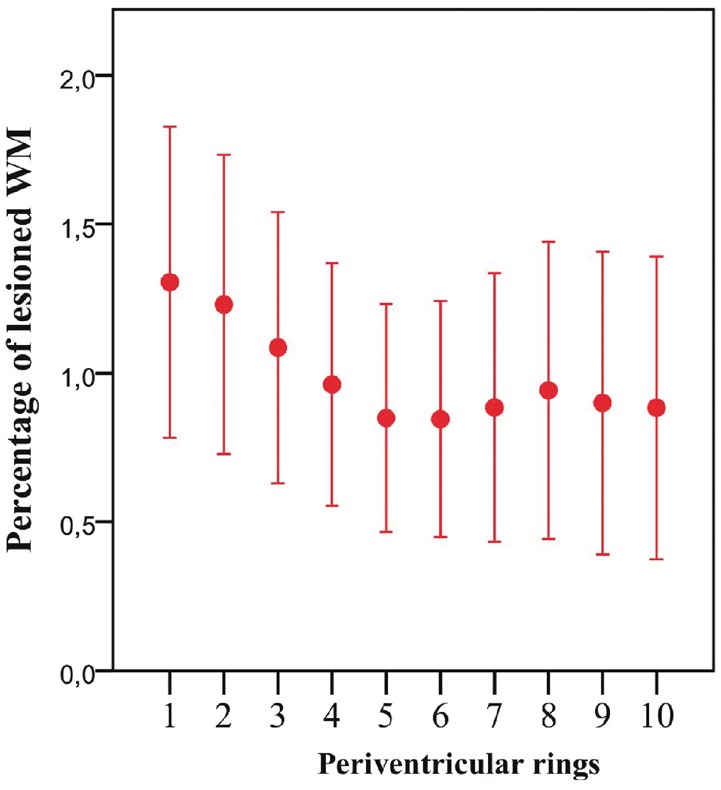
In established multiple sclerosis, tissue abnormality-as assessed using magnetization transfer ratio-increases close to the lateral ventricles. We aimed to determine whether or not (i) these changes are present from the earliest clinical stages of multiple sclerosis; (ii) they occur independent of white matter lesions; and (iii) they are associated with subsequent conversion to clinically definite multiple sclerosis and disability. Seventy-one subjects had MRI scanning a median of 4.6 months after a clinically isolated optic neuritis (49 females, mean age 33.5 years) and were followed up clinically 2 and 5 years later. Thirty-seven healthy controls (25 females, mean age 34.4 years) were also scanned. In normal-appearing white matter, magnetization transfer ratio gradients were measured 1-5 mm and 6-10 mm from the lateral ventricles. In control subjects, magnetization transfer ratio was highest adjacent to the ventricles and decreased with distance from them; in optic neuritis, normal-appearing white matter magnetization transfer ratio was lowest adjacent to the ventricles, increased over the first 5 mm, and then paralleled control values. The magnetization transfer ratio gradient over 1-5 mm differed significantly between the optic neuritis and control groups [+0.059 percentage units/mm (pu/mm) versus -0.033 pu/mm, P = 0.010], and was significantly steeper in those developing clinically definite multiple sclerosis within 2 years compared to those who did not (0.132 pu/mm versus 0.016 pu/mm, P = 0.020). In multivariate binary logistic regression the magnetization transfer ratio gradient was independently associated with the development of clinically definite multiple sclerosis within 2 years (magnetization transfer ratio gradient odds ratio 61.708, P = 0.023; presence of T2 lesions odds ratio 8.500, P = 0.071). At 5 years, lesional measures overtook magnetization transfer ratio gradients as significant predictors of conversion to multiple sclerosis. The magnetization transfer ratio gradient was not significantly affected by the presence of brain lesions [T2 lesions (P = 0.918), periventricular T2 lesions (P = 0.580) or gadolinium-enhancing T1 lesions (P = 0.724)]. The magnetization transfer ratio gradient also correlated with Expanded Disability Status Scale score 5 years later (Spearman r = 0.313, P = 0.027). An abnormal periventricular magnetization transfer ratio gradient occurs early in multiple sclerosis, is clinically relevant, and may arise from one or more mechanisms that are at least partly independent of lesion formation.
Keywords: magnetization transfer ratio; multiple sclerosis; normal-appearing white matter.
© The Author (2016). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Adams CW, Abdulla YH, Torres EM, Poston RN. Periventricular lesions in multiple sclerosis: their perivenous origin and relationship to granular ependymitis. Neuropathol Appl Neurobiol 1987; 13: 141–52. - PubMed
-
- Alcazar A, Regidor I, Masjuan J, Salinas M, Alvarez-Cermeno JC. Axonal damage induced by cerebrospinal fluid from patients with relapsing-remitting multiple sclerosis. J Neuroimmunol 2000; 104: 58–67. - PubMed
-
- Andeweg J. The anatomy of collateral venous flow from the brain and its value in aetiological interpretation of intracranial pathology. Neuroradiology 1996; 38: 621–8. - PubMed
-
- Barker GJ, Tofts PS, Gass A. An interleaved sequence for accurate and reproducible clinical measurement of magnetization transfer ratio. Magn Reson Imaging 1996; 14: 403–11. - PubMed
-
- Barkhof F, Filippi M, Miller DH, Scheltens P, Campi A, Polman CH, et al.Comparison of MRI criteria at first presentation to predict conversion to clinically definite multiple sclerosis. Brain 1997; 120 (Pt 11): 2059–69. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
