

Transanal total mesorectal excision (TaTME) for rectal cancer: effects on patient-reported quality of life and functional outcome
- PMID: 28044239
- PMCID: PMC5285410
- DOI: 10.1007/s10151-016-1570-z
Transanal total mesorectal excision (TaTME) for rectal cancer: effects on patient-reported quality of life and functional outcome
Abstract
Background: Transanal total mesorectal excision (TaTME) has rapidly become an important component of the treatment of rectal cancer surgery. Cohort studies have shown feasibility concerning procedure, specimen quality and morbidity. However, concerns exist about quality of life and ano(neo)rectal function. The aim of this study was to prospectively evaluate quality of life in patients following TaTME for rectal cancer with anastomosis.
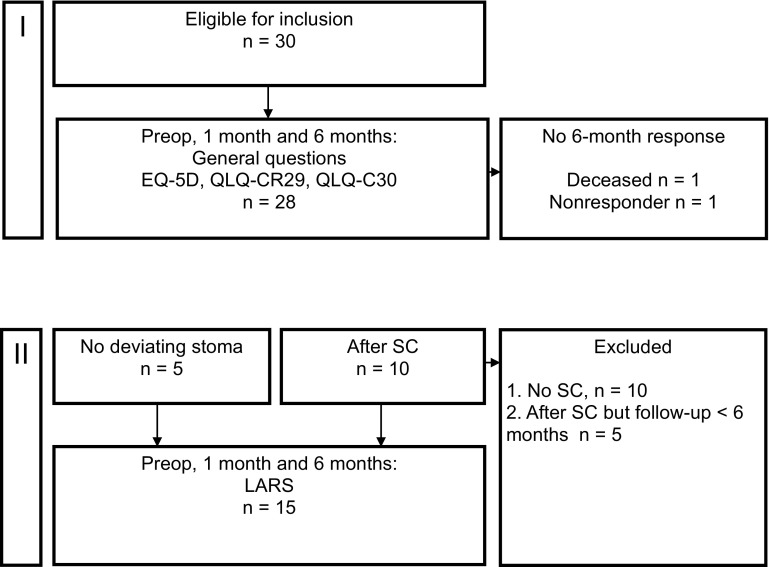
Methods: Consecutive patients who underwent restorative TaTME surgery for rectal adenocarcinoma in an academic teaching center with tertiary referral function were evaluated. Validated questionnaires were prospectively collected. Quality of life was assessed by the EuroQol 5D (EQ-5D), European Organization for Research and Treatment of Cancer's QLQ-C30 and QLQ-CR29 and low anterior resection syndrome (LARS) scale. Outcomes of the questionnaires at 1 and 6 months were compared with preoperative (baseline) values.
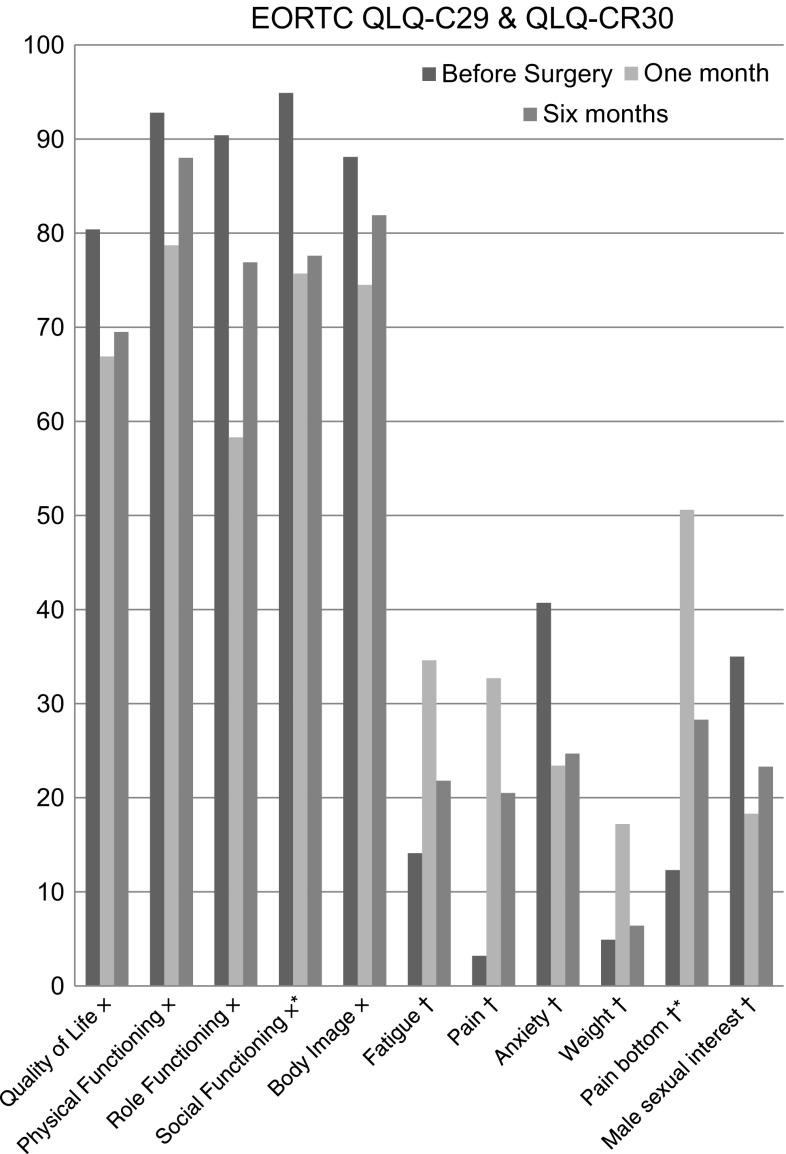
Results: Thirty patients after restorative TaTME for rectal cancer were included. Deterioration for all domains was mainly observed at 1 month after surgery compared to baseline, but most outcomes had returned to baseline at 6 months. Social function and anal pain remained significantly worse at 6 months. Major LARS (score >30) was 33% at 6 months after ileostomy closure. No end colostomies were required.
Conclusions: TaTME is associated with acceptable quality of life and functional outcome at 6 months after surgery comparable to published results after conventional laparoscopic low anterior resection.
Keywords: Cancer; PROMs; Quality of life; Rectum; Surgery; TaTME.
Conflict of interest statement
The authors declare that they have no conflict of interest. Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. We are pleased to confirm that the Medical Research Involving Human Subjects Act (WMO) does not apply to the above-mentioned study and that an official approval of this study by our committee is not required. The Medical Ethics Review Committee of VU University Medical Center is registered with the US Office for Human Research Protections (OHRP) as IRB00002991. The FWA number assigned to VU University Medical Center is FWA00017598. Informed consent Informed consent was obtained from all individual participants included in the study.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
