

Oncologic Procedures Amenable to Fluorescence-guided Surgery
- PMID: 28045715
- PMCID: PMC6280663
- DOI: 10.1097/SLA.0000000000002127
Oncologic Procedures Amenable to Fluorescence-guided Surgery
Abstract
Objective: Although fluorescence imaging is being applied to a wide range of cancers, it remains unclear which disease populations will benefit greatest. Therefore, we review the potential of this technology to improve outcomes in surgical oncology with attention to the various surgical procedures while exploring trial endpoints that may be optimal for each tumor type.
Background: For many tumors, primary treatment is surgical resection with negative margins, which corresponds to improved survival and a reduction in subsequent adjuvant therapies. Despite unfavorable effect on patient outcomes, margin positivity rate has not changed significantly over the years. Thus, patients often experience high rates of re-excision, radical resections, and overtreatment. However, fluorescence-guided surgery (FGS) has brought forth new light by allowing detection of subclinical disease not readily visible with the naked eye.
Methods: We performed a systematic review of clinicatrials.gov using search terms "fluorescence," "image-guided surgery," and "near-infrared imaging" to identify trials utilizing FGS for those received on or before May 2016.
Inclusion criteria: fluorescence surgery for tumor debulking, wide local excision, whole-organ resection, and peritoneal metastases.
Exclusion criteria: fluorescence in situ hybridization, fluorescence imaging for lymph node mapping, nonmalignant lesions, nonsurgical purposes, or image guidance without fluorescence.
Results: Initial search produced 844 entries, which was narrowed down to 68 trials. Review of literature and clinical trials identified 3 primary resection methods for utilizing FGS: (1) debulking, (2) wide local excision, and (3) whole organ excision.
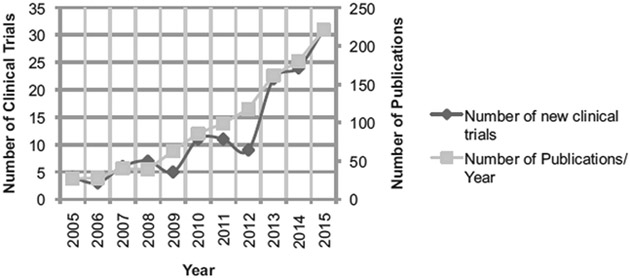
Conclusions: The use of FGS as a surgical guide enhancement has the potential to improve survival and quality of life outcomes for patients. And, as the number of clinical trials rise each year, it is apparent that FGS has great potential for a broad range of clinical applications.
Figures





References
-
- Stummer W, Pichlmeier U, Meinel T, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol. 2006;7:392–401. - PubMed
-
- Rizzo M, Iyengar R, Gabram SG, et al. The effects of additional tumor cavity sampling at the time of breast-conserving surgery on final margin status, volume of resection, and pathologist workload. Ann Surg Oncol. 2010;17:228–234. - PubMed
-
- Tartter PI, Kaplan J, Bleiweiss I, et al. Lumpectomy margins, reexcision, and local recurrence of breast cancer. Am J Surg. 2000;179:81–85. - PubMed
-
- Singletary SE. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg. 2002;184:383–393. - PubMed
